Sacral nerve sparing strategy in carbon-ion irradiation of pelvic sarcomas: the MedAustron approach
Ankita Nachankar,
Austria
MO-0946
Abstract
Sacral nerve sparing strategy in carbon-ion irradiation of pelvic sarcomas: the MedAustron approach
Authors: Ankita Nachankar1,2, Eugen Hug1, Maciej Pelak1, Slavisa Tubin1, Markus Stock3,4, Antonio Carlino4, Joanna Gora4, Giovanna Martino4, Mansure Schafasand4,5, Piero Fossati1,6
1MedAustron Ion Therapy Center, Austria, Radiation Oncology, Wiener Neustadt, Austria; 2ACMIT Gmbh, Austria, Research & Development in Medical Technology, Wiener Neustadt, Austria; 3Karl Landsteiner University of Health Sciences, Austria, Medical Physics, Krems an der Donau, Austria; 4MedAustron Ion Therapy Center, Austria, Medical Physics, Wiener Neustadt, Austria; 5Medical University of Vienna, Austria, Radiation Oncology, Wien, Austria; 6Karl Landsteiner University of Health Sciences, Austria, Radiation Oncology, Krems an der Donau, Austria
Show Affiliations
Hide Affiliations
Purpose or Objective
Purpose/Objective: Carbon-ion therapy (CIRT) is a potentially curative treatment for inoperable pelvic sarcomas/chordomas. A possibly debilitating side-effect of pelvic hypofractionated CIRT is Radiation-Induced Lumbosacral Neuropathy (RILSN), if doses to nerves >70Gy RBE. At present no clear recommendations are available for sacral nerve sparing optimized (SNSo) CIRT treatment planning. The purpose of this study is to evaluate the feasibility of SNSo-CIRT plans and correlate it with initial, preliminary clinical outcomes data.
Material and Methods
Material/Methods: We contoured individual nerve roots at L4–S3 levels until they converge to the sciatic nerves (figure 1a). CIRT plans with pencil beam scanning (PBS) were optimized with local effect model -I (LEM) (Europe) to calculate relative biological effectiveness (RBE)-weighted doses. To validate dose distributions of SNSo-CIRT plans across different RBE models, doses were recalculated using the modified microdosimetric kinetic model (mMKM) (NIRS, Japan-scanning beam). Prescription doses were (LEM) of 73.6 (64-76.8) Gy RBE in 16 fractions of 4-4.8 Gy RBE, (4 fractions/ week). Doses to nerves outside of high dose clinical target volume (HD-CTV) were limited to D2% <69 or <73 Gy RBE and hot spots were avoided on nerves inside HD-CTV. Robustness of SNSo-CIRT plans were evaluated against different range and set-up uncertainty scenarios.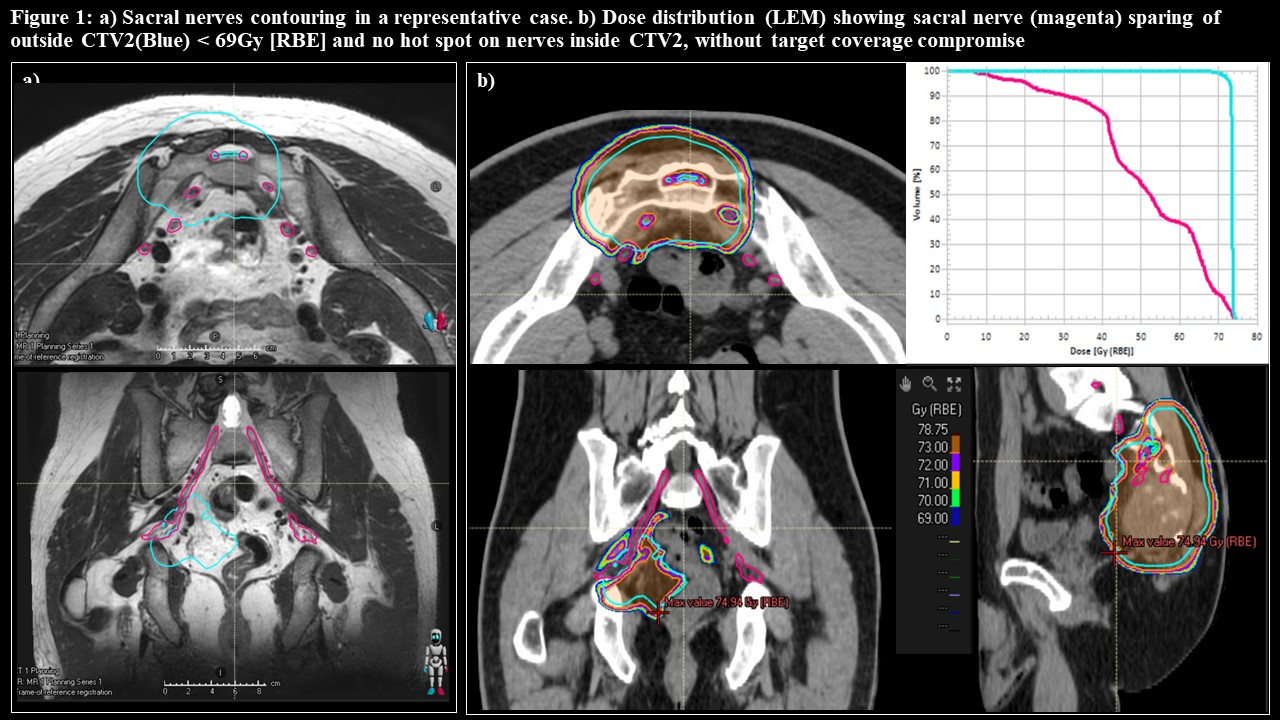
Results
Results: Twenty patients with pelvic sarcomas/chordomas treated with CIRT at MedAustron from November 2020 to February 2022 were analyzed. Median follow up was 11.4 months (range, 4.6-25.3). Majority of patients had sacral chordomas (17/20). Sharper penumbra, smaller spot of carbon-ions and PBS technique permitted to limit doses to sacral nerves without significantly compromising target dose coverage (figure 1b). SNSo-CIRT plans were feasible in all patients and robustly optimized against different scenarios. Early follow-up revealed a cumulative incidence of RILSN (grade 1-3) of 15.7% at 2-years. Two (10%) patients developed grade 3 RILSN (CTCAE v5). Median time to develop RILSN was shorter, 4.8 months (range, 2-6)., partly because of curettage surgery for sacral chordoma in one and type II diabetes in another. Higher average maximum doses, Dmax to sacral nerves (76.41 +/- 3.78 vs 68.63 ± 25.24 Gy RBE) and dose to 2cc of nerves, D2cc (71.42 ± 1.19 vs 64.27 ± 23.71 Gy RBE) were observed on mMKM recalculation in RILSN patients (Table 1). Log rank test showed, (LEM) D0.5cc, D1cc and D2% as significant predictors Actuarial 1-year local control rate was 95% and none of the local recurrences could be correlated to nerve sparing strategy. None developed other grade >2 toxicities.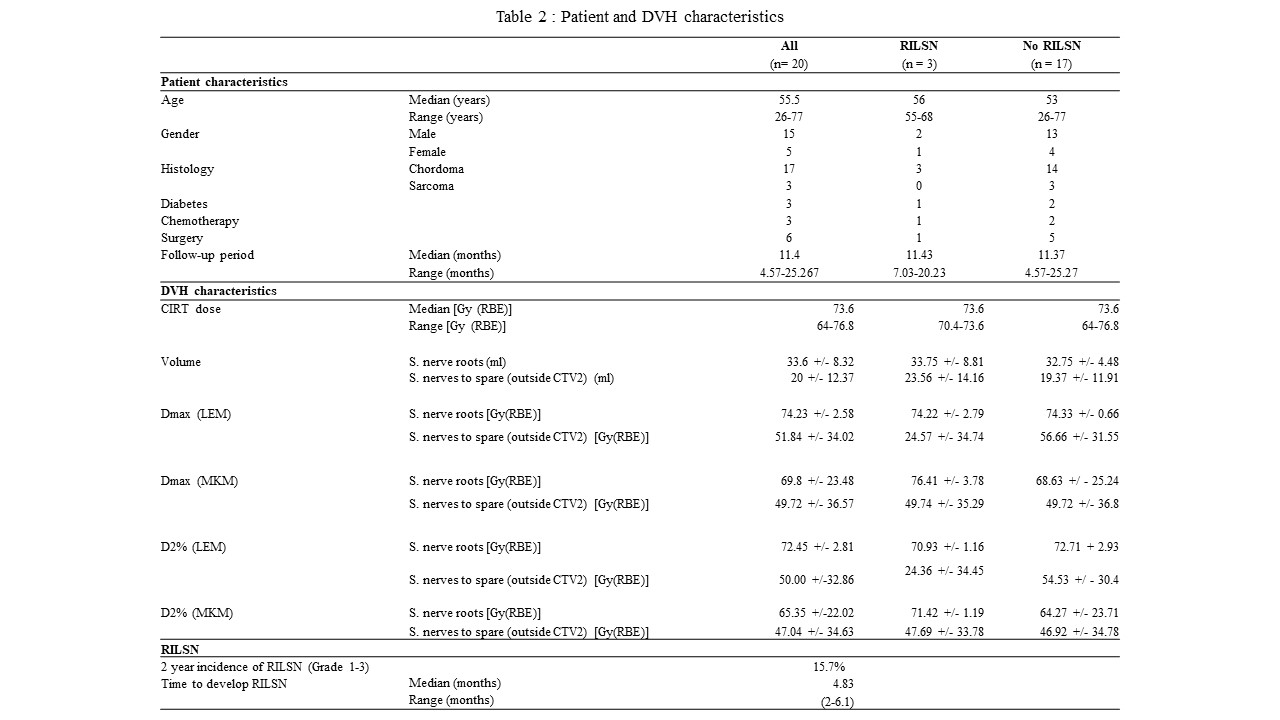
Conclusion
Conclusion: RILSN is a potentially serious long-term toxicity. Our preliminary data suggest that sacral nerve sparing is technically feasible and could minimize RILSN. Longer follow up is required to establish local control and RILSN risk analysis. The optimal dose constraints have still to be determined.