partial brachytherapy in prostate cancer phantoms with and without rectum spacer
PO-1819
Abstract
partial brachytherapy in prostate cancer phantoms with and without rectum spacer
Authors: Ben Vanneste1, Vassilious Skouteris2, Louis Campos Pinheiro3, Nelson Stone4
1Maastro, Radiotherapy Oncology, Mastricht, The Netherlands; 2Hygeia Hospital, Urology, Athens, Greece; 3Hospital da Luz, Urology, Lisboa, Portugal; 4The Icahn School of Medicine at Mount Sinai New York, Urology and Radiation Oncology, New York, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
To determine different approaches of focal
brachytherapy with and without rectum spacer derived in an in-vitro prostate
cancer simulation.
Material and Methods
Two
different focal strategies are examined: a lateralized approach (left-right)
and the both posterior lobes strategy, which is the predominant position of a
clinically significant prostate cancer. Two sets of implants were used in an in-vitro
study using the Simulated Inanimate Models of prostate with a dominant lesion (Gross
tumor volume, GTV)(SIMTM): the loose Mick seeds in comparison with
the linked stranded I125 seeds. The prescribed dose to the clinical
target Volume (CTV), and the GTV were at least 200 Gy. Furthermore a rectum
spacer (barrigel®) was injected to decrease the dose to the rectum. Post-implant
Computed Tomographies of the phantoms were performed with a post-implant dosimetry.
The rectum D1cc and D2cc were compared
with and without spacer implant.
Results
The focal volumes of the CTV varied from 5
to 15 cc (mean 8 cc, the percentages of ‘‘focal volume/whole prostate volume’’
varied between 17% and 38% with a mean of 26%). The focal volumes of GTV varied
from 0.7 to 1 cc. The total number of
needles necessary to implant the focal volume varied between 7 and 10 (mean, 9).
The total number of seeds (activity 0.500 to 0.600 mCi) varied from 27 to 41
(mean, 33). The mean focal D90 of GTV and CTV were 273 Gy (range, 195 Gy –
434Gy) and 227 Gy (range, 168-277 Gy). The D90 for the entire prostate gland
was 60.8 Gy (range, 32.6 - 111 Gy). No differences were observed between loose
or stranded technique.
On average, 12.5 mm separation was achieved
between the prostate and the rectum (range, 11-14 mm). The mean doses to 1 cc
of rectum (D1cc), and the mean doses to 2 cc of rectum (D2cc) without spacer
vs. with spacer were 40.2% vs. 24.4%, 33.8% vs. 24.9% , and 48.9 Gy vs. 36.2 Gy, respectively. 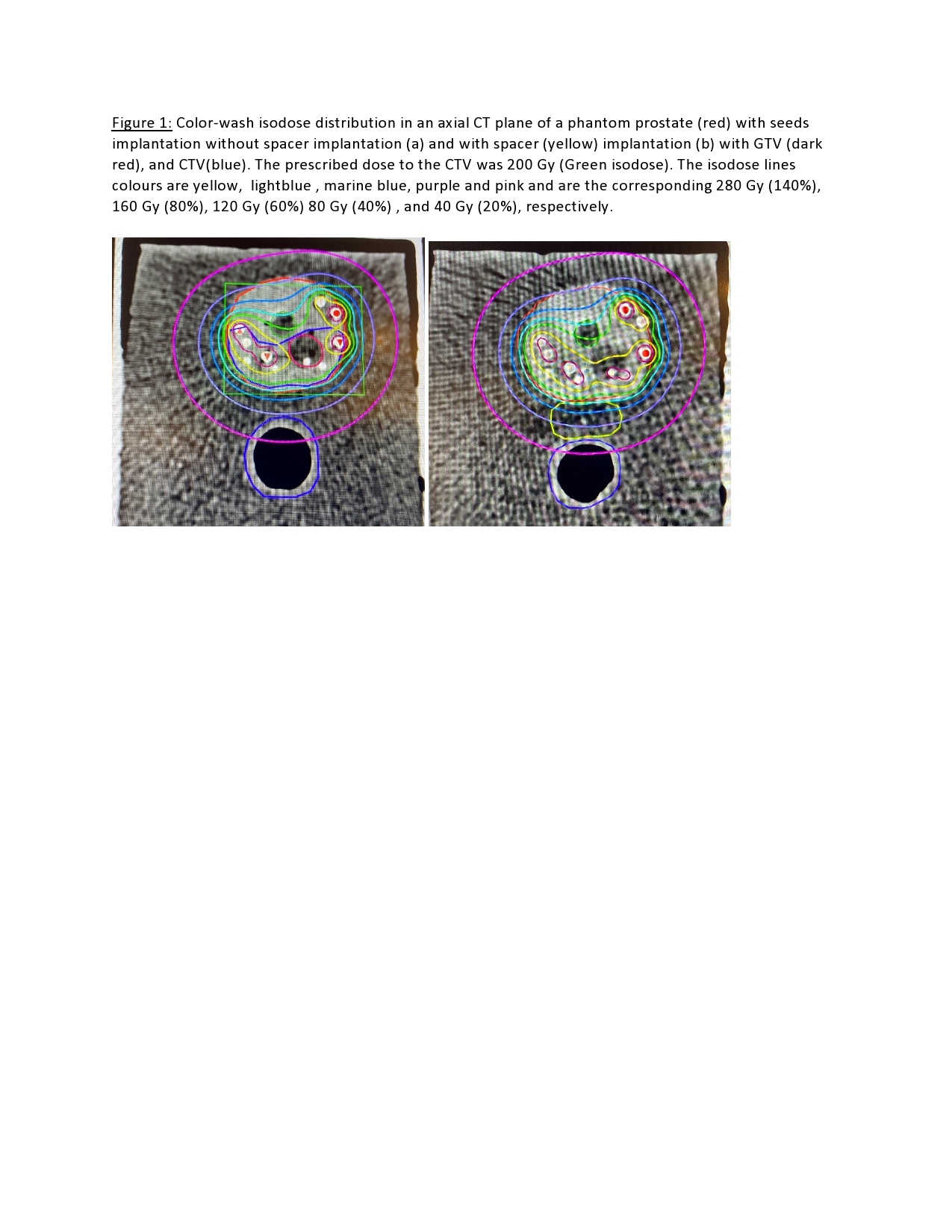
Conclusion
The
prescription of doses above 200 Gy and the implantation of seeds in the clinical
significant region for focal therapy in phantoms are feasible. All rectal
dosimetric parameters improved for the spacer implants as compared with the non-spacer
implants. Further clinical validation of this concept is warranted.