Low Dose Radiation Therapy for COVID-19 Pneumonia: Risk of Cancer with AP-PA fields and IMRT
PO-1561
Abstract
Low Dose Radiation Therapy for COVID-19 Pneumonia: Risk of Cancer with AP-PA fields and IMRT
Authors: Daya Nand Sharma1, Seema Sharma1, Anil Gupta1, Vellaiyan Subramani1, Surendra Saini1, KP Haresh1, Rambha Pandey1
1All India Institute of Medical Sciences, New Delhi, Radiation Oncology, New Delhi, India
Show Affiliations
Hide Affiliations
Purpose or Objective
Low dose radiation therapy (LDRT) to lungs has
shown encouraging results in patients with Covid-19 pneumonia. Though the
prescribed dose of LDRT is very low (0.5-1.5 Gy), but there has been some concern
regarding the risk of radiation induced carcinogenesis (RIC). Risk is dependent
on the amount of radiation exposure and the age at exposure. Most LDRT trials
have used conventional AP-PA open fields. Modern technique like IMRT can
potentially reduce the organs at risk (OAR) doses thereby minimizing the risk
of RIC. We designed a dosimetric study to see if IMRT can reduce the dose to OARs
and lessen the risk of RIC in Covid-19 patients.
Material and Methods
We retrieved the CT scan data
of 10 patients who have been already treated for any malignancy in the region
of thorax. The following selection
criteria were used 1) Age >40 years 2) equal number of male and female
patient so as to estimate the risk of RIC in breast 3) no previous surgery in
the thoracic area and intact thoracic organs and breast 4) complete set of CT imaging from mandible to L1vertebra. The
CT data of each patient was used to delineate the CTV and OAR to generate two parallel
plans: one with open fields (Conventional Plan) and one with VMAT. A dose of 1
Gy in single fraction was prescribed to PTV which included both lungs. Mean OAR
doses were used to estimate the risk of RIC for both plans and compared. The excess relative risk (ERR) of RIC was estimated
using online radiation risk assessment calculator (https://irep.nci.nih.gov/radrat). This tool (RadRT) uses the risk models broadly
based on Biological Effects of Ionizing Radiation (BEIR) VII with some modifications. The ERR
values the two plans were compared. For
statistical analysis, two tailed Wilcoxon
signed rank test was used to
compare the dosimetry and ERR between two planning techniques. A p-value of
<0.05 was considered significant.
Results
The beam-on time and monitor units (MU) were
less with conventional plan but all other DVH parameters (D95, Dmean, CI and HI) were
significantly better with VMAT (p value <0.05 for all). Mean dose to most
OAR like esophagus, spinal cord, thyroid and skin was significantly lower with
VMAT (p value <0.05 for all). Mean heart dose with conventional plan was not
only higher than VMAT plan (<0.05)
but also crossed the prescribed dose. Table
1 shows the comparison of ERR in both the plans. The overall ERR is significantly lower with VMAT as compared to
conventional plan (0.357 vs 0.398%, p value <0.05). The ERR for all individual organs except thyroid was
significantly lower with VMAT. Even though the mean thyroid dose was
significantly less with VMAT than conventional plan, but the ERR for thyroid
cancer was comparable with two plans. ERR was significantly less with VMAT. In both
plans, the ER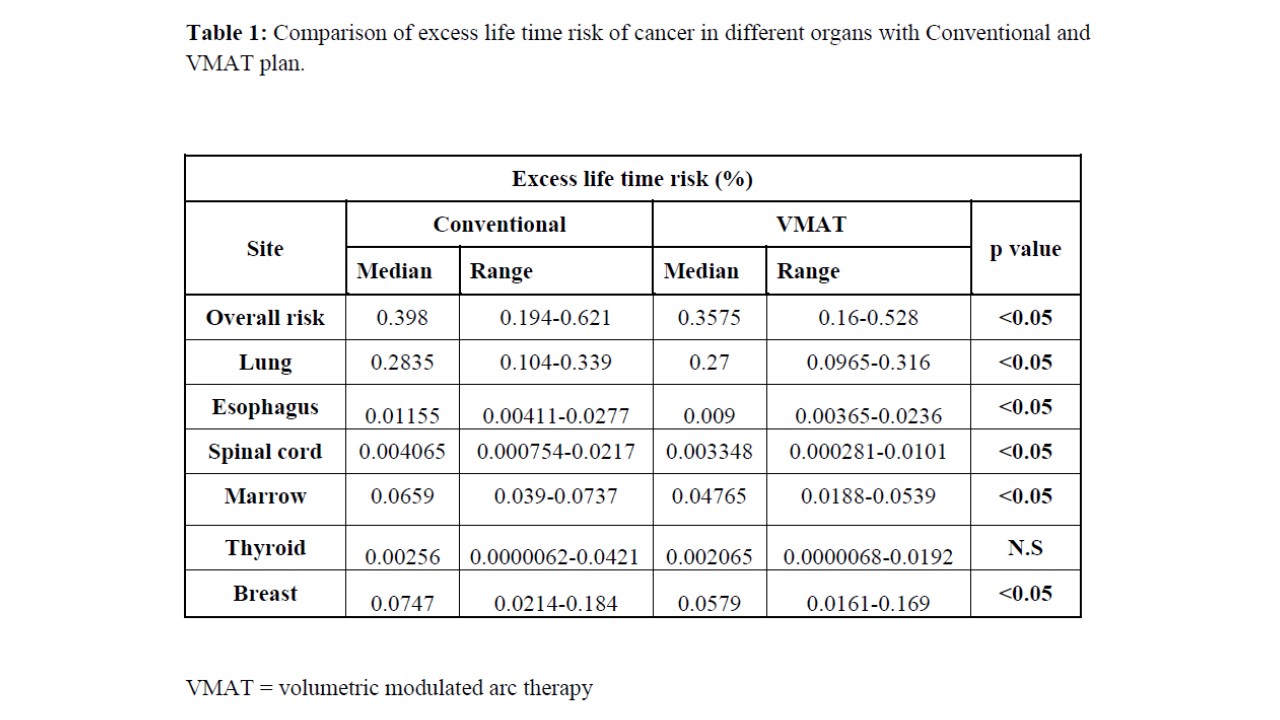 R was highest for lung followed by breast and marrow.
R was highest for lung followed by breast and marrow.
Conclusion
Our dosimetric study shows that IMRT can lessen
the risk of RIC in Covid-19 patients undergoing LDRT.