Accuracy of a skull based automatic 6D match with kV-kV imaging on a Truebeam
Sjoerd Hoek,
The Netherlands
PO-2270
Abstract
Accuracy of a skull based automatic 6D match with kV-kV imaging on a Truebeam
1Amsterdam UMC, Radiotherapy, Amsterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Set-up of brain indications at our department consisted of orthogonal kV-kV imaging with a 4D manual bone match based on the skull. On the Truebeam (Varian Medical systems), it is technically possible to use an automatic 6D bone match with kV-kV set-up though this was not tested yet.
For a 6D set-up, CBCT could also be considered. This would expose patients to a higher imaging radiation dose and cost more time compared to kV-kV imaging. The necessity to see soft tissue with brain indications is mostly negligible: CBCT image quality rarely suffices to differentiate the PTV from other brain tissue.
If the accuracy of an automatic 6D kV-kV match is comparable to a CBCT match on the skull, it would improve a manual 4D match. Matches would be faster and more accurate without using more radiation for imaging.
The aim of this study is to compare the accuracy of a 6D kV-kV vs 6D CBCT automatch on the bony structures of the skull.
Material and Methods
For this study 19 brain and sinus patients with 411 fractions in a 5-points thermoplastic mask(MacroMedics) were included as well as 102 intracranial stereotactic patients with 304 fractions in a frameless mask(Brainlab).
An automatic 6D kV-kV match was applied followed by a 6D CBCT automatch. The data from 6D match on CBCT was analyzed to verify any accuracy differences of the 6D kV-kV match. All matches were based on skull structures only.
Literature suggests that 6D couch usage can result in residual errors. A significant correlation between performed roll and lateral residual errors and to a lesser extent a performed pitch and longitudinal residual errors is proven. This can be minimized through fixation (Guckenberger et al. 2007).
Since frameless masks are more rigid, these were examined separately from the 5-points masks in order to filter out any stability differences.
Results
Fig. 1 shows lateral residual errors >1.5 mm with 5-points masks are only seen when roll >1° is applied, this correlation is significant(r = -0.74). With frameless masks these residual errors are not that prominent nor significant(r = -0.21).
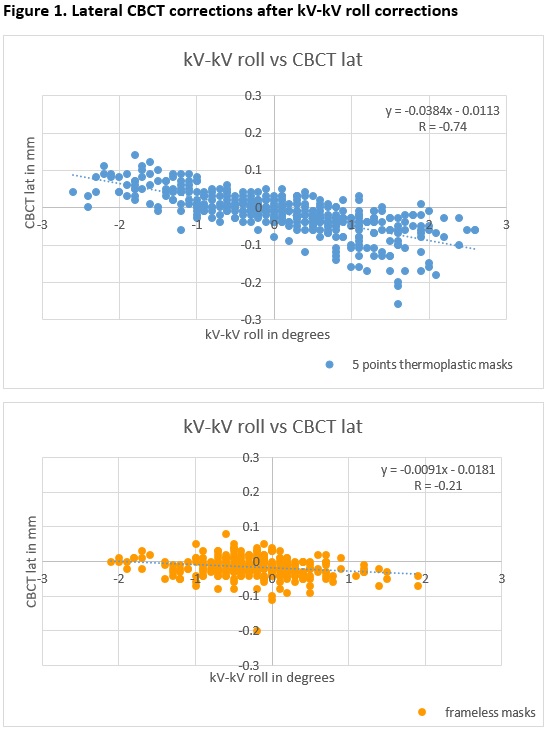
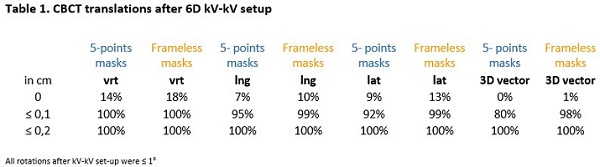
Table 1 shows that after a 6D kV-kV match with 5-points masks, 100% of the lateral and longitudinal residual errors are ≤ 0.2 cm. All vertical residual errors were ≤0.1cm and all rotational residual errors were ≤ 1°.
The residual errors seen with the 5-points masks are not seen with the frameless masks due to the stability difference of the masks. This indicates a intrafraction movement after performing a roll or pitch and not an inaccurate 6D kV-kV match.
Conclusion
Small shifts in the CBCT match after a performed kV-kV match are caused by a performed roll or pitch and not by a difference between the kV-kV and CBCT algorithm.
Using 6D kV-kV imaging based on skull structures seems feasible for clinical use. Although it is advised to check for residual errors after a performed pitch/roll with a certain margin.