The importance of spot distribution and its influence on the LEM/MKM model relationship in CIRT
PO-1985
Abstract
The importance of spot distribution and its influence on the LEM/MKM model relationship in CIRT
Authors: Joanna Gora1, Piero Fossati1,2, Marta Mumot1, Muhammad Shamshad1, Markus Stock1,2, Antonio Carlino1
1MedAustron Ion Therapy Center, Medical Department, Wiener Neustadt, Austria; 2Karl Landsteiner University of Health Sciences, -, Krems, Austria
Show Affiliations
Hide Affiliations
Purpose or Objective
Carbon ion radiotherapy (CIRT) has been clinically employed in different centers with different RBE models (mostly LEM or MKM). Although many LEM/MKM translation strategies are already used in clinical routine to convert dose prescriptions and OARs dose constraints, there are many factors (not only model, but also treatment planning related) that can influence the LEM/MKM relationship. This study focus on spot distribution strategies and its influence on the translation between the models.
Material and Methods
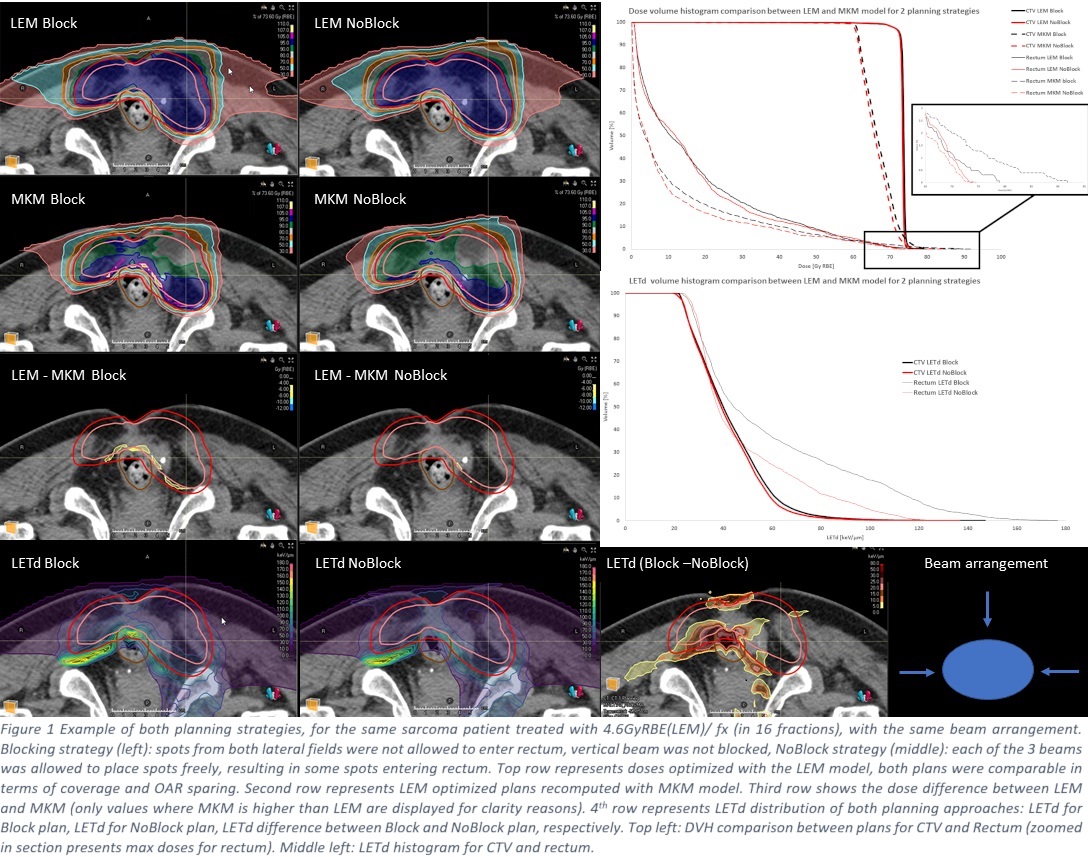
20 patients with various indications and tumor sites, previously treated with CIRT were selected. They followed protocols derived from the Japanese experience and adjusted for the different RBE model (4.1-4.8 Gy RBE/fx). Prescription and OAR constraints were translated from MKM RBE-weighed doses (obtained from clinical data) into LEM. All clinical plans had between 2-4 beams, spaced at least by 30◦. They were clinically optimized with LEM model, implemented in RayStation11B (RaySearch Laboratories) and subsequently recomputed with the MKM (the physical doses remain identical). Additionally, the LETd distribution was evaluated. 2 main strategies of treatment planning were considered: a) Blocking: placement of the spots was not allowed in the certain regions (forbidding beams going through OARs to reach the contralateral portion of the target); b) NoBlocking: spots could be placed freely, each beam could have contribution in the whole volume. Both sets of plans were comparable in terms of LEM dose distribution, having similar coverage and OARs sparing.
Results
Results were consistent for all examined plans as exemplified in fig1. As expected, plans recomputed in MKM resulted generally in lower doses comparing to LEM optimized plans. Detailed evaluation showed that strategy b) achieved MKM maximum doses to OAR (rectum in the case shown) similar to LEM (72.5vs73.5 Gy RBE, respectively), while scenario a) resulted in higher doses to OAR after recomputation (92vs79 Gy RBE), exceeding the OARs constraints. Areas of increased MKM doses was also consistent with higher LETd values (reflected in the LETd histogram, rectum V10% increased from 80keV/µm to almost 120keV/µm).
Conclusion
Spot distribution and therefore beam contribution has a major influence on the LEM/MKM translations and they should be included in the planning strategy, especially when escalation of the OARs is considered. Blocking allows reducing mid and low dose in the blocked OAR, but may result in worse MKM and LETd distribution. It still might be still required in certain situations, but the planner needs to be aware of the limitations: fulfilling LEM constraints does not mean that MKM constraints will automatically be respected. Special care is required, especially when OARs are in proximity of the blocked regions. Moreover, the study highlights the need for implementation of additional tools in commercial systems (i.e. RBE dose visualization per beam, SFO, LETd optimization,etc) to allow safer and optimal CIRT treatment.