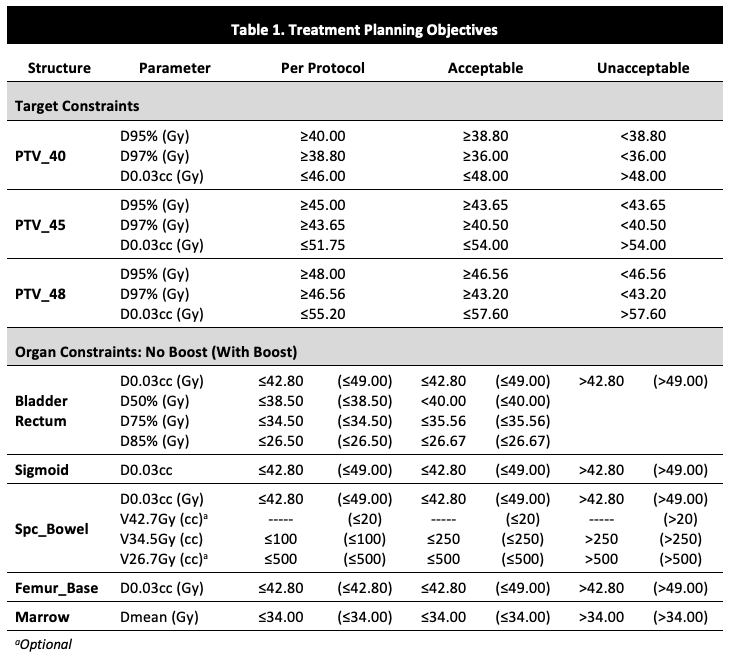
The HYACINCT protocol defines a set of guidelines for image acquisition, target and organ delineation and treatment planning objectives (Table 1).
Fifteen dummy cases were prepared, five each for three levels of dose requirements: 40Gy without boost, and with boost to 45Gy and to 48Gy. IMRT and VMAT plans were prepared for each case, evaluated and assigned penalty and compliance scores according to planning objectives, and subjected to quality control.
IMRT and VMAT plans were created by the same physicist for each case using the Eclipse® v. 16.1 (Varian Medical Systems) treatment planning system (TPS) for a Varian VitalBeam® linear accelerator, using 6-MV photons. For the IMRT plan, a single isocenter and seven evenly-spaced coplanar beams were employed. Sliding-window multi-collimator leaf motion was used. For the VMAT plan, the isocenter was placed at the same location similar to that of the IMRT plan. Two full-rotation arcs and collimator angles 45° and/or 315° were used.
IMRT and VMAT plans were compared in terms of treatment plan quality (target coverage, penalty and compliance scores), and treatment delivery. Tumor extent (T-stage, T-score), nodal status, and PTV volumes (in cc) were examined as potential determinants of penalty and compliance scores.