Impacts of mechanical errors on dose distributions and control quality results for VMAT plans
Christophe Legrand,
France
PO-1706
Abstract
Impacts of mechanical errors on dose distributions and control quality results for VMAT plans
Authors: Christophe Legrand1, Maryline Posnic1, Damien Autret1, Jean-Marc Fontbonne2, Cathy Fontbonne3, Stéphane Dufreneix1
1Integrated Center for Oncology, Medical Physics, Angers, France; 2Normandie University, ENSICAEN, CNRS/IN2P3, LPC Caen, Caen, France; 3Normandie University, ENSICAEN, CNRS/IN2P3, LPC Caen, Angers, France
Show Affiliations
Hide Affiliations
Purpose or Objective
The aim of this work was to investigate the consequences of systematic mechanical errors on selected dosimetric indicators and gamma-pass rate (GPR) results with portal imager for three accelerators.
Material and Methods
Ten patients treated with VMAT for H&N cancer were randomely selected. Dose distribution calculations and pre-treatment acquisitions were performed on a TrueBeam (MLC 120), a TrueBeam STx (MLC HD120) and a Halcyon. Eight plans per patient were created to study the impact of changes in 4 parameters that could each be set at three levels: all banks A and B MLC leaves shifted (-1 mm, 0 mm, +1 mm), gantry and collimator (-1°, 0°, +1°). This experimental design included the two most unfavorable presupposed cases in terms of dose impact: plans with all leaves shifted to +1 mm (“All opened plan (AOP)”) and shifted to -1 mm (“All closed plan (ACP)”). Studied indicators were: relative dose differences of PTV (D95%), parotids and thyroid (Dmean), spinal cord (D2%); 2D GPR<1 using three Global/Local Absolute gamma criteria: GA2%/3mm, LA2%/3mm, LA2%/2mm. A multiple linear regression (MLR) was performed to estimate the influence of each mechanical parameter on studied indicators for each patients.
Results
MLR results suggested: gantry and collimator errors as non-significant factors (up to 1° shift); MLC systematic error as a significant influencing factor on dose deviations with a significant interaction between MLC banks. For all accelerators and each organ studied, doses differences are given Figure 1 for both AOP and ACP: median doses deviations were greater than 5% for all organs at risk. For PTV, a median dose deviation of about 5% for a systematic error of ±1 mm was pointed out. Measurements with portal imager were performed on the Halcyon. The AOP gave mean 2D GPR between TPS calculations and portal acquisitions equal to 92.5% (GA2%/3mm, without error: 100%), 89.7% (LA2%/3mm, without error: 99.9%), 73.9% (LA2%/2mm, without error: 99.6%). These first results suggested that LA2%/2mm criteria had the best sensibility to MLC systematic errors as GPR from GA2%/3mm and LA2%/3mm gamma criteria had a majority of GRPs above 90% (Figure 2).
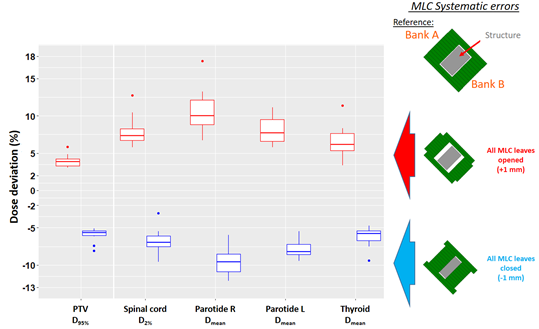
Figure 1: Doses deviations (%) for PTV and OARs between plan without error and both worst cases
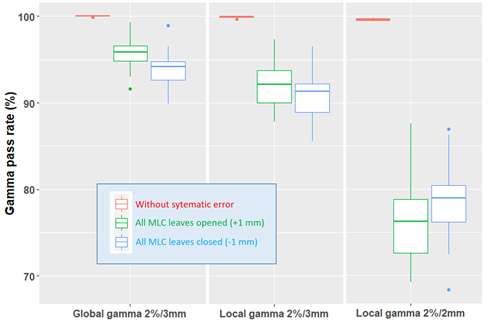
Figure 2: Halcyon’s Gamma pass rates (%) for various tolerance criteria
Conclusion
MLC systematic errors influenced significantly dose deviations to PTV and OARs: an increase of about 1% for D95% PTV can be caused by a 0.2 mm systematic shift of MLC leaves bank. 2D GPR results for Halcyon had a good sensibility to MLC systematic positioning errors at the gamma criteria LA2%/2mm while the other criteria gave values above 90%. Works are in progress: to study the dosimetric impacts on conformity/homogeneity indices and the 3D GPR of each organ; to perform portal imager measurements on the TrueBeam and TrueBeam STx; to analyze the correlations between the results of pretreatment controls and all these dosimetric indices combined with a predictive approach.