Validation of iMAR algorithm usage through dosimetric comparisons of iMAR vs MDO in different TPS
CELINE KARLA TORZSOK,
Chile
PO-1680
Abstract
Validation of iMAR algorithm usage through dosimetric comparisons of iMAR vs MDO in different TPS
Authors: CELINE KARLA TORZSOK1, Alvaro Ruiz2, Marcelo Ribeiro2, Filippo Marangoni3, Jhonalbert Aponte2, Rixy Plata2, Matias Pino2, Jose Luis Rodriguez2, Herve Broque2
1Falp Fundacion Arturo Lopez Perez, radiation Therapy, Santiago, Chile; 2Falp Fundacion Arturo Lopez Perez, Radiation Therapy, Santiago, Chile; 3Falp Fundacion Arturo Lopez Perez,, Radiation Therapy, Santiago, Chile
Show Affiliations
Hide Affiliations
Purpose or Objective
Artefacts caused by metal implants are one of the challenges to deal with in RT both during structures contouring and treatment planning calculations especially when target volumes are close to metal implants. Evenwhen there are methodologies to reduce the artefacts impact in TPS, like, using a tissue dependent Manual Density Override (MDO) or applying artefact reduction algorithms, there are no comparisons between these practices. Some CT scanners propose a solution to the problem described through artefact reduction algorithms . This work presents a set of tests performed on the iMAR algorithm (iterative Metal Artefact Reconstruction) to evaluate its impact on HU, absorbed dose in RT plans for different calculation algorithms and machines, and additionally, a dosimetric (point dose and Gamma analisis) comparison of iMAR with MDO as a validation methodology prior to implementing iMAR in our clinical practice.
Material and Methods
For the evaluation of the iMAR algorithm, this work was divided into three parts. First was evaluation of the HU generated by iMAR in a CIRS 062M phantom carrying metal inserts to create artefacts in the image. Then, through measures we assessed the dosimetric impact when iMAR was applied. In the end, a dosimetric comparison between different treatment plans and different TPS was made in order to estimate changes with respect to MDO. For the measurements, we used a Standard Imaging A1SL ionisation chamber with a Tomoelectrometer and a Gammex Cheese Phantom with metal inserts to create artefacts. The TPSs evaluated were Monaco (Elekta), Precision and Tomoplanning (Accuray) and Eclipse (Varian).
Results
After application of the iMAR algorithm in the CIRS phantom with artefacts, the HU values retrieved were in accordance with those of the same phantom without artefacts (maximum difference was 98 HU) (figure 1). The noise in the resulting image was slightly higher in the processed image.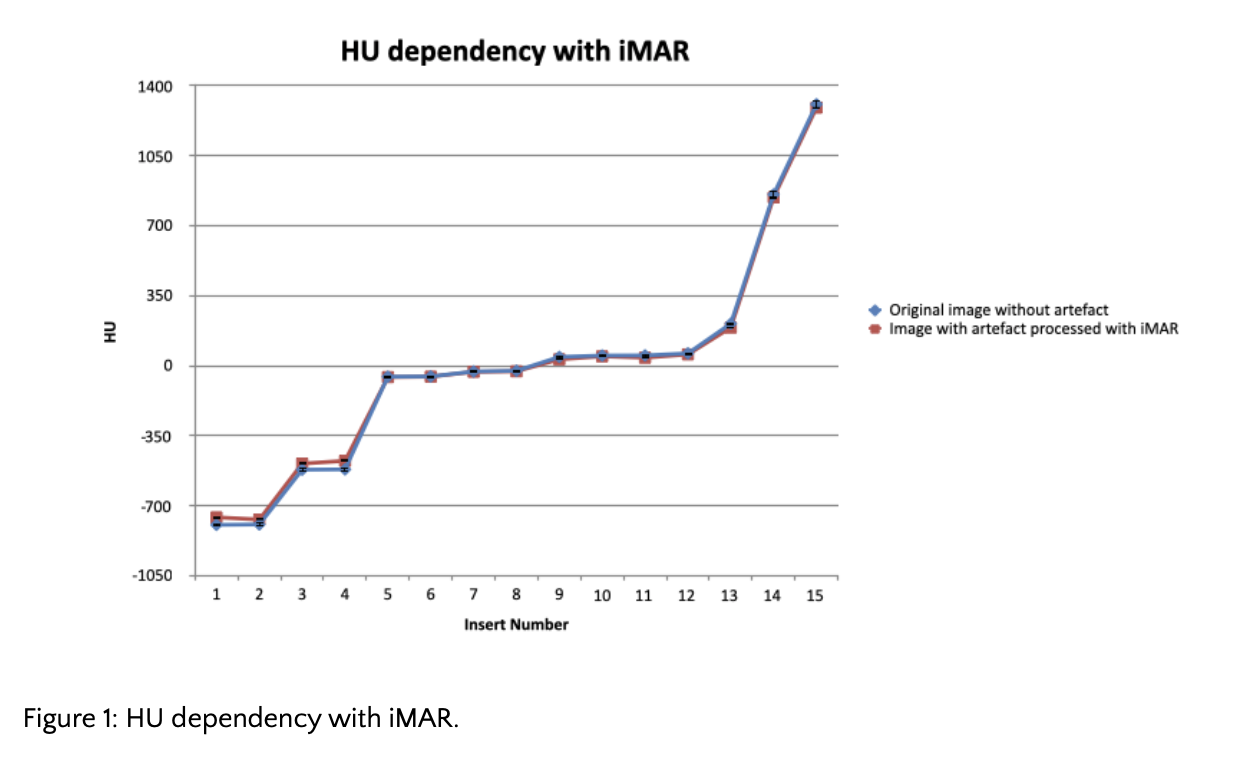 The maximum dose difference between measurements in the different machines and TPSs calculation was +2% and -1% for iMAR and MDO, respectively.
The maximum dose difference between measurements in the different machines and TPSs calculation was +2% and -1% for iMAR and MDO, respectively.
Dosimetric comparisons of iMAR vs MDO in different TPSs show similar values of absorbed dose even in cases where the artefact occupied one third or more of the of prescription dose volume. Figure 2 shows a case of bilateral hip prosthesis where Gamma analysis was 99% (2%, 2 mm, 10% threshold).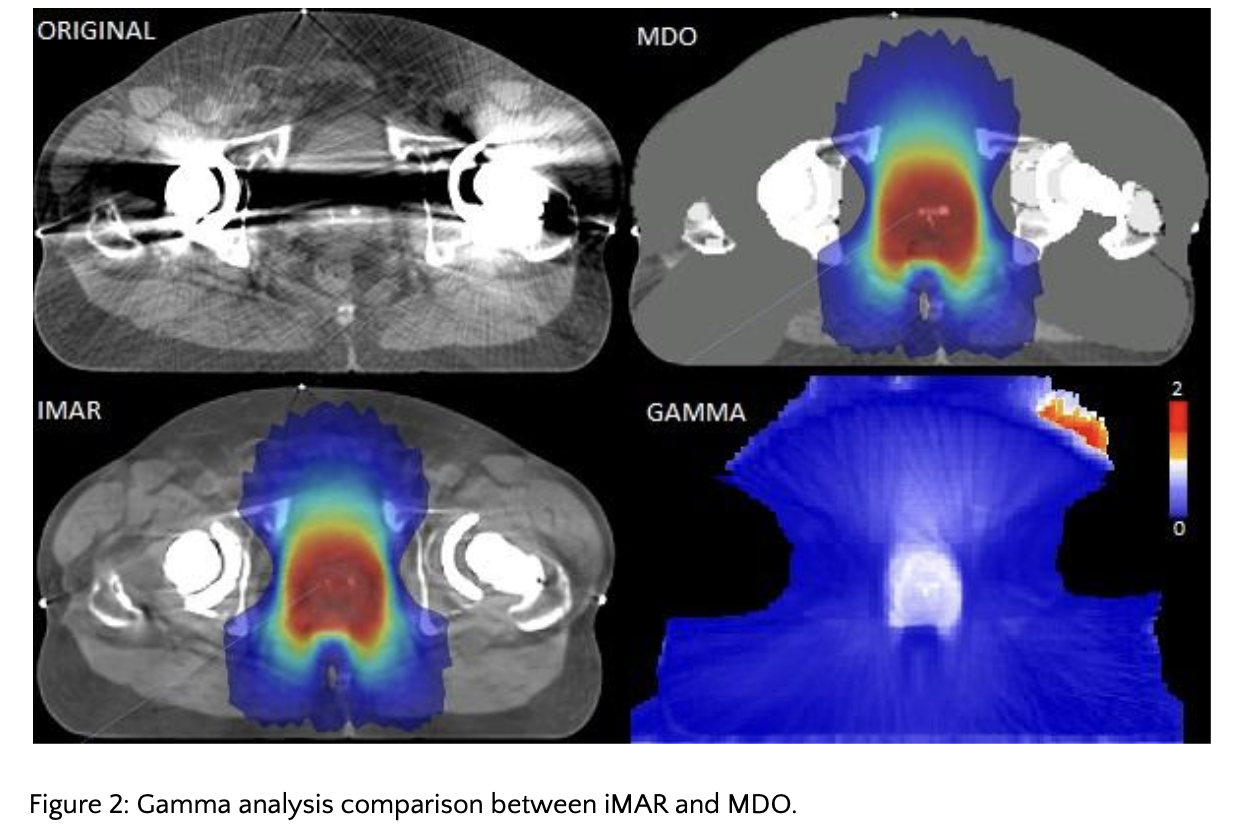
Conclusion
iMAR usage was validated even when artefacts caused by metallic implants are high. It allows for a better representation of the dose in comparison with MDO. Also, iMAR improves the clinical workflow, decreasing the chance of mistakes and saving time during treatment planning. In cases where CT scanners do not provide iMAR, there remains the option to apply MDO, thus lowering the dose difference due to artefacts to less than 5%.