Stereoscopic radiographic IGRT and thermo-optical SGRT for DIBH breast radiotherapy
PO-1902
Abstract
Stereoscopic radiographic IGRT and thermo-optical SGRT for DIBH breast radiotherapy
Authors: Martin Buschmann1, Daniela Kauer-Dorner1, Stefan Konrad1, Dietmar Georg1, Joachim Widder1, Barbara Knäusl1
1Department of Radiation Oncology, Comprehensive Cancer Center Vienna, Medical Imaging Cluster, Medical University of Vienna/AKH Wien, Vienna, Austria
Show Affiliations
Hide Affiliations
Purpose or Objective
The deep inspiration breath hold (DIBH) manoeuvre for breast cancer radiotherapy requires accurate and reproducible patient positioning and motion monitoring. The novel ExacTrac Dynamic 1.1 (ETD) positioning system (Brainlab AG, Munich) combines thermo-optical surface imaging (SGRT) with in-room-based stereoscopic X-ray IGRT and was recently released with a dedicated breast DIBH workflow. While portal imaging (EPID) and cone-beam CT (CBCT) are well established modalities for breast IGRT, the performance of stereoscopic X-rays in this setting is unknown. IGRT data utilizing the dedicated DIBH ETD workflow of the first six breast cancer patients was retrospectively analyzed.
Material and Methods
For left-sided patients with breast cancer two planning CTs were acquired: one in free-breathing (FB) and one in DIBH, with patients immobilised via a breast board. The surface contours of both CTs were extracted to derive the DIBH amplitude and a ±2.5 mm breathing window was added. Treatments were prescribed as whole breast radiotherapy (40 Gy in 15 fx) with a sequential boost to the tumor bed (10 Gy in 4 fx) and were delivered by 3DCRT, IMRT, or VMAT. Before each fraction, patients were pre-positioned based on the FB surface information. Once the visually guided DIBH position was reached, two stereoscopic X-ray images were acquired and registered to the left-sided ribs on digitally reconstructed radiographs (DRR) derived from the DIBH CT. Based on the registration a 6 DOF couch correction was performed to re-position the patient. Positioning and monitoring by ETD were verified by established EPID or CBCT imaging based procedures at selected fractions. Residual geometric deviations detected by EPID/CBCT verification imaging were analyzed but not corrected for.
Results
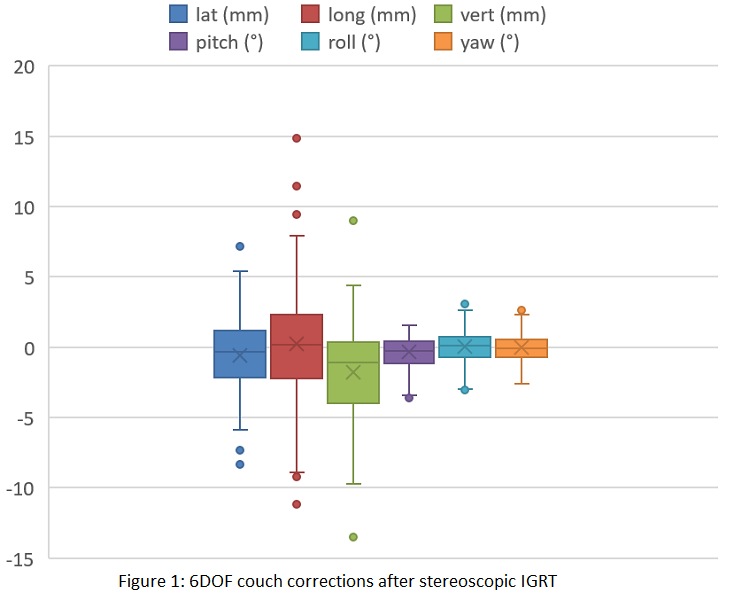
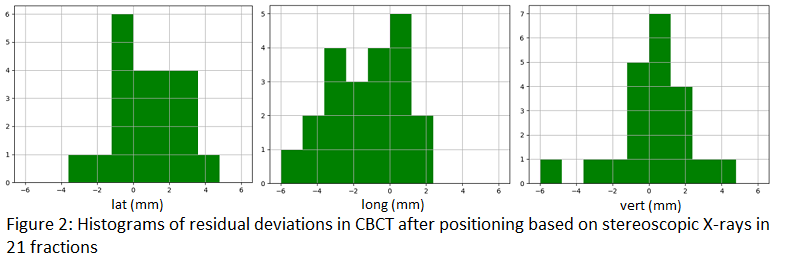
Six DIBH breast patients were treated in 99 fractions using ETD for SGRT+IGRT. The mean X-ray derived couch correction vector from the FB surface position to DIBH X-ray location was 5.7±3.5 mm (see Figure 1), while the correlation between these values was weak (R=0.31–0.51 for 3 translations). A good correlation (0.77-0.82) was observed between the surface signal and X-ray position in the same breathing status, namely DIBH. Verification imaging was performed for 32 fractions (53 RT field verifications) with EPID and for 21 fractions with CBCT, respectively. The mean 2D/3D deviation vector length over all verification images was 2.5±1.4 mm / 3.4±1.7 mm for EPID/CBCT (see Figure 2), both measures were well within the PTV margins (7 mm). Surface monitoring was challenging for larger patients and low breast board inclination.
Conclusion
DIBH treatments with the ETD system combining SGRT and stereoscopic IGRT were feasible. The successful verification of the ETD X-ray positioning by standard IGRT techniques paved the way for clinical implementation. The cause of residual deviations – systematic differences between the imaging modalities or the limited reproducibility of the DIBH manoeuvre – remains subject for further investigations.