Gated dynamic trajectory radiotherapy: feasibility, mechanical accuracy and dosimetric validation
Hannes Anton Loebner,
Switzerland
PO-1893
Abstract
Gated dynamic trajectory radiotherapy: feasibility, mechanical accuracy and dosimetric validation
Authors: Hannes Anton Loebner1, Daniel Frauchiger1, Dario Terribilini1, Silvan Mueller1, Gian Guyer1, Paul-Henry Mackeprang1, Marco Francesco Mario Stampanoni2, Michael Karl Fix1, Peter Manser1, Jenny Bertholet1
1Inselspital, Bern University Hospital and University of Bern, Division of Medical Radiation Physics and Department of Radiation Oncology, Bern, Switzerland; 2ETH Zuerich and PSI, Institute for Biomedical Engineering, Villigen, Switzerland
Show Affiliations
Hide Affiliations
Purpose or Objective
By extending VMAT with dynamic table and collimator rotation during beam-on, dynamic trajectory radiotherapy (DTRT) has shown improved organ at risk sparing compared to VMAT. To deliver the intended dose distribution to a moving anatomy, motion mitigation, e.g. by gating, can be applied. However, this may be a challenge due to the increase in dynamic degrees-of-freedom of DTRT. The aim of this work is to experimentally assess the technical feasibility, quantify the mechanical accuracy and validate the dosimetric performance of respiratory gating during DTRT delivery.
Material and Methods
An HexaMotion motion stage with a Delta4 phantom positioned on the treatment table of a TrueBeam system is used to mimic four different breathing motion traces: typical, high frequency, predominantly left-right and baseline shift, each with combined motion in superior-inferior, anterior-posterior, and left-right directions.
A DTRT plan for a clinically motivated lung case is delivered both with and without gating in developer mode on a TrueBeam system. For gating, the real-time positioning management (RPM) system is used to trigger amplitude gating based on the main motion axis (either superior-inferior or anterior-posterior) with gating window between 4 and 6 mm depending on the motion trace.
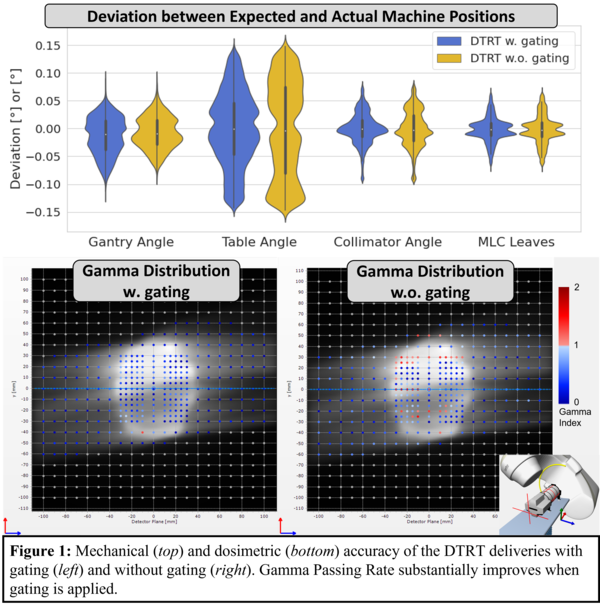
Mechanical accuracy is assessed from TrueBeam trajectory log files as the deviation between actual and expected machine positions for gantry, table and collimator angle and positions of moving MLC leaves. Dosimetric accuracy is determined by comparing the calculated dose to the measured dose using the Delta4 phantom by means of the gamma analysis (3% global/2 mm, 10% threshold). Additionally, the dosimetric accuracy is assessed for a DTRT delivery and a static phantom.
Results
DTRT delivery was successfully gated with the gantry, table and collimator rotating back during beam-hold and resuming motion at beam-on (i.e., when entering the gating window). The deviation between expected and actual machine position for deliveries with and without gating are shown in figure 1. The spread of the mechanical deviations is slightly smaller for deliveries with gating, which is believed to be related to the reset of lagging machine components at gating events. Deliveries with gating (resp. without) achieved gamma passing rates >96% (<88%) (figure 1). For the static phantom, the passing rate was 99%.
Conclusion
DTRT was successfully delivered with gating on a TrueBeam system for the first time. Machine accuracy was similar to delivery without gating. Gating substantially improved the dosimetric plan quality as compared to deliveries without gating.
This work was partially supported by Varian Medical Systems.