Is beam gating needed for MR-guided SBRT of adrenal gland metastases?
PO-1888
Abstract
Is beam gating needed for MR-guided SBRT of adrenal gland metastases?
Authors: Uffe Bernchou1,2, Anders Bertelsen1, Tine Schytte1,2, Carsten Brink1,2, Faisal Mahmood1,2
1Odense University Hospital, Department of Oncology, Odense, Denmark; 2University of Southern Denmark, Department of Clinical Research, Odense, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
MR-guided radiotherapy of abdominal and thoracic targets could potentially benefit from the use of respiratory beam gating. This study aims to investigate the potential improvement in target dose coverage if beam gating is used for adaptive MR-guided SBRT of adrenal gland metastases.
Material and Methods
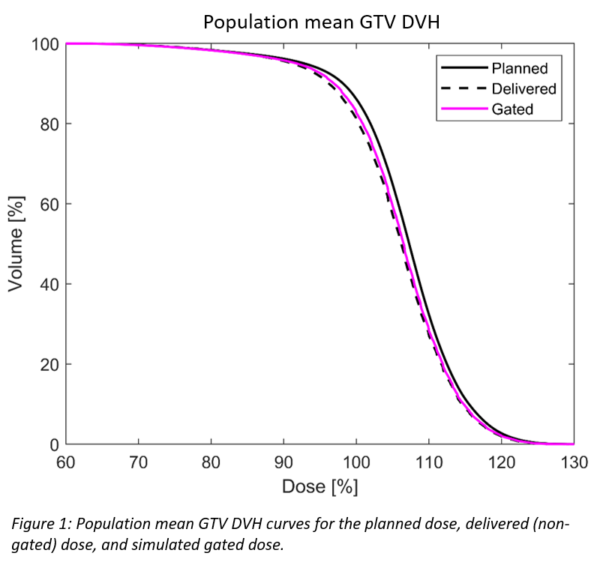
The study includes 31 patients with adrenal gland metastases treated on a 1.5 T MR linac without beam gating options to 45 Gy in 3 fx (n=12), 50 Gy in 5 fx (n=17), or 60 Gy in 8 fx (n=2). Dose planning aimed to achieve a conformal and inhomogeneous dose distribution maximising the GTV V95% and mean dose, and covering the PTV with 67% of the prescribed dose while respecting hard OAR constraints. The PTV margins were based on the peak-to-peak respiration target motion assessed on pre-treatment 4DCT. Patients were treated while breathing freely (n=14), or with breathing motion restricted by the use of an abdominal compression belt (n=17). 2D interleaved coronal and sagittal cine MR images were acquired at 5 Hz during treatment. These images were analysed using an in-house tracking algorithm to obtain the time-resolved position of the target. The delivered GTV dose was estimated from the daily planned dose that was rigidly shifted and accumulated according to the time-resolved target position changes due to drift and respiration motion. To simulate gating, beam hold was triggered when 5% of a 2D projected GTV was outside a gating window of GTV+3 mm. The dosimetric consequences of motion were summarised by a population mean GTV DVH, and by changes in V95% and mean GTV dose compared to the planned dose.
Results
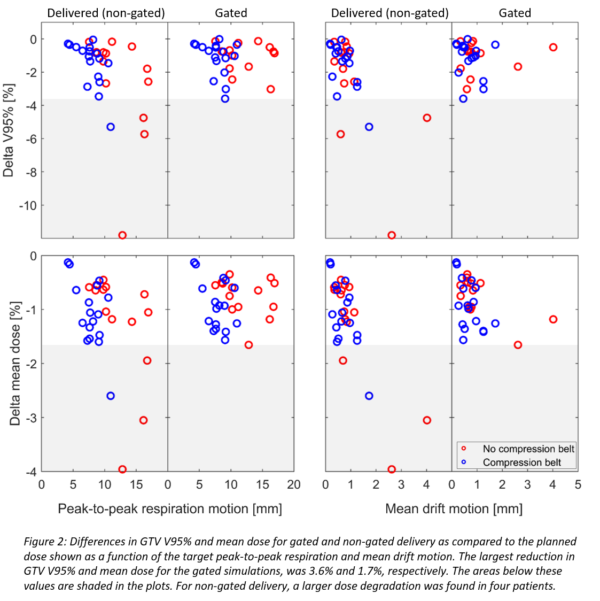
During simulated gating, the median (range) beam hold time was 5% (0%-70%) of the treatment time. The population mean DVH curves for the planned, delivered, and GTV dose using simulated gating is shown in figure 1. The use of gating would only result in a modestly higher GTV dose than what was delivered without gating. Figure 2 shows the per patient differences in GTV V95% and mean dose for gated and non-gated delivery as compared to the planned dose. The differences are shown as a function of the target peak-to-peak respiration and mean drift motion during treatment delivery. Relative to the planned dose, the largest reduction in GTV V95% and mean dose in any patient was 3.6% and 1.7%, respectively, for the gated simulations. For non-gated delivery, a larger dose degradation was found in four patients. These patients exhibited either a large target drift or respiration motion. However, only one of these four patients had breathing motion restricted by a compression belt.
Conclusion
Despite a swift dose fall-off outside the GTV, the use of beam gating during SBRT of adrenal gland metastases treated on an MR linac would not lead to clinically relevant improvement in target coverage for most patients. Only one patient out of 17 treated with a compression belt would have benefitted from the use of beam gating.