The effect of Monte Carlo uncertainty in daily online plan adaptation
PO-1878
Abstract
The effect of Monte Carlo uncertainty in daily online plan adaptation
Authors: Thyrza Jagt1, Tomas Janssen1, Jan-Jakob Sonke1
1Netherlands Cancer Institute, Department of Radiation Oncology, Amsterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Monte Carlo (MC) based treatment planning systems use a pre-set statistical uncertainty to determine the number of particle histories to be calculated. A lower uncertainty results in more accurate dose distributions but also higher calculation times. In clinical practice, a statistical uncertainty of 1% per plan is common.
In daily online adaptive radiotherapy, treatment plan adaptation has to be performed as fast as possible, raising the question whether MC uncertainty can be increased. In particular, in fractionated treatments, the noise due to a high MC uncertainty may average out over the full treatment. This study evaluates the effect of higher MC uncertainty for online adaptive plan adaptation.
Material and Methods
We evaluated four MC uncertainty values: 1% (the clinical value), 2%, 3% and 5%. For 20 prostate cancer patients the planning scans were used to generate reference plans (5x7.25Gy ). To investigate the effect of daily plan adaptations, we sampled five rigid shifts from a normal distribution with mean 0 and SD=5mm for each patient in all directions. Plans were reoptimized on the 5 corresponding shifted planning scans using the online adaptation workflow in Monaco (Elekta). All plans optimized with a MC uncertainty >1% were recalculated using a 1% uncertainty for comparison purposes.
For each patient we calculated the D98% and D2% for the PTV, and the D2% and Dmean for the Bladder and Rectum, for all 5 fractions and for each MC uncertainty. For each parameter the 5 values per patient were averaged to get an estimate of each accumulated dose parameter. These average values were compared to the 1% uncertainty fraction plan values per patient.
Results
Boxplots of the normalized differences between the average dosimetric parameter values per higher MC uncertainty value and the average dosimetric parameter value of the 1% uncertainty fraction plan per patient are shown in Fig_1. It can be seen that almost all differences are between -2% and 2%, with the exception for the Bladder and Rectum Dmean. This could be due to the objective functions used in the planning, where high doses were more emphasized than mean doses.
In general the PTV parameters as well as the Bladder D2% were reduced a little in median with respect to the adapted plan with 1% uncertainty, while the Bladder Dmean and Rectum parameters increased a little.
For the PTV dosimetric parameters, only small increases in the difference values can be seen when using a higher MC uncertainty value, resulting in a median increase of 0.5% for the PTV D98%.
When comparing the different uncertainty values, little variation is observed.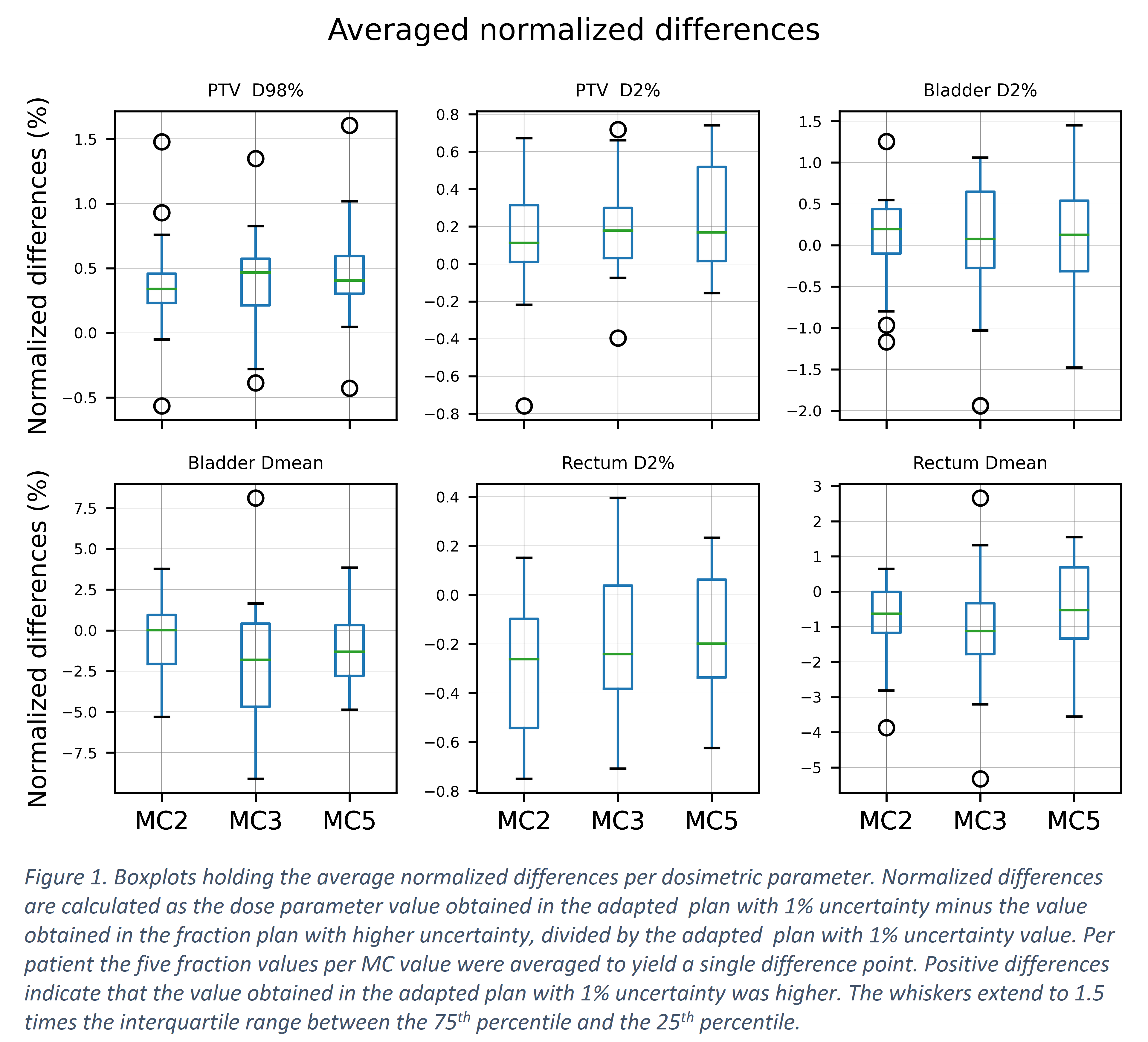
Conclusion
This study shows that when dealing with rigid full body translations for prostate cancer patients, daily plan adaptation using a higher MC uncertainty value can lead to small differences with respect to an adapted plan with 1% uncertainty. Increasing the uncertainty from 2% to 5% has minimal effect suggesting that faster plan adaptations may be feasible.