Assessment of setup errors and internal motion for rectal cancer using MR-guided radiotherapy
PO-1872
Abstract
Assessment of setup errors and internal motion for rectal cancer using MR-guided radiotherapy
Authors: Tim Everaert1, Adrian Gutierrez Ruiz1, Randa Atef Kamel1, Jacques Bodenst Bezuidenhout1, Jelle Smeulders1, Thierry Gevaert1, Mark De Ridder1
1UZ Brussel, Radiotherapy, Brussels, Belgium
Show Affiliations
Hide Affiliations
Purpose or Objective
Short-term preoperative radiotherapy with a simultaneous integrated boost on the tumor with or without concomitant chemotherapy is accepted as standard of care for T3-T4 rectum treatment before total mesorectal excision. The use of MR guided radiotherapy offers better soft tissue visualization, real-time intrafraction motion monitoring and online adaptive planning when needed, potentially leading to the reduction of treatment margins. The aim of this work was to assess the setup errors and internal motion of patients treated for rectal cancer with MR-guided radiotherapy.
Material and Methods
Ten patients underwent treatment on the MRIdian® (Viewray) for rectum carcinoma in five fractions of 5 Gy with a simultaneous boost of 6 Gy per fraction on the GTV. In total 44 fractions were analyzed. For every fraction, an extra post-treatment MR sequence (TrueFISP) was acquired. Intrafraction patient movement was analyzed via a rigid fusion of pre-and post-treatment MR. To calculate internal motion the movement of the mesorectum and GTV was analyzed over the course of the treatment.
Results
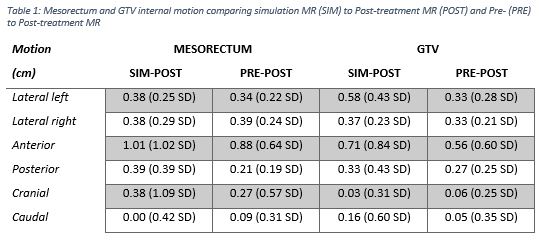
Rigid fusion analysis of the pre- and post-treatment scans shows a mean of the absolute values of 0.94 mm ± 0.98 SD in lateral, 1.26 mm ± 1.31 SD in vertical and 0.75 mm ± 0.62 SD in longitudinal direction. No rotational movement bigger than 1.68° was found. This suggests that patient position during treatment is stable. The internal movements of the mesorectum and GTV comparing simulation to post-treatment MR and pre- to post-treatment MR are shown in table 1. Intrafractional internal motion of the mesorectum and GTV was found consistently lower when compared to interfractional motion (simulation vs post-treatment scan).
Conclusion
The use of MR-guided radiotherapy with smaller margins is plausible for the treatment of rectal cancer. This novel technique provides a way to determine setup errors and internal motion by bringing confidence due to real time imaging and online adaptation. This allows adaptation of the currently used treatment margins.