Dose adaptive radiotherapy: Compensating for target motion without PTV margins
Erik van der Bijl,
The Netherlands
PO-1866
Abstract
Dose adaptive radiotherapy: Compensating for target motion without PTV margins
Authors: Erik van der Bijl1, Jan-Jakob Sonke2, Peter Remeijer2, Uulke van der Heide2, Tomas Janssen2
1Radboudumc, Department of Radiation Oncology, Nijmegen, The Netherlands; 2The Netherlands Cancer Institute, Department of Radiation Oncology, Amsterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
The introduction of daily online plan adaptation is motivated by its potential to reduce planning target volume (PTV) margins. However, daily online adaptation also allows the dose distribution to be adjusted every treatment fraction to compensate for geometrical inaccuracies in the previous fractions. In this work, we studied the potential benefit of daily dose adaptation as an alternative for PTV margins.
Material and Methods
We considered two adaptation strategies, where we assume that the accumulated target dose so far is known and that random (σ) and systematic (Σ) Gaussian geometric errors of the population are known. In both strategies the first N-1 fractions are planned with 0 mm margin, while the last fraction has an isotropic margin of 2.5√(Σ^2+σ^2 ) to ensure geometric coverage during the last fraction. In the first strategy we accumulated the dose after N-1 fractions to determine the required (inhomogeneous and anisotropic) dose distribution in the last fraction, to arrive at the desired dose coverage of the CTV. The second strategy updates the planned dose after each fraction.
As a proof of principle, we considered an idealized spherically symmetric target and dose distribution characterized by a Gaussian penumbra σp=3.2 mm and we simulated N=5 fraction treatments based on Gaussian geometric errors characterized with random error σ={0.5, 1.0, 1.5, 2.0} mm and systematic error Σ = 1 mm in all directions. We implemented dose accumulation by a subdivision of the CTV in 24 segments with equal solid angles, the local planned dose in each sector is calculated from the minimal accumulated dose in this segment.
We assessed the accumulated target coverage, target inhomogeneity and mean dose in a 1 cm ring around the CTV, and compared this with the classical situation with a fixed PTV margin and a homogeneous prescription dose to the PTV.
Results

Figure 1: Boxplot of planned CTV Dmax of all simulated treatments for the two adaptation strategies.
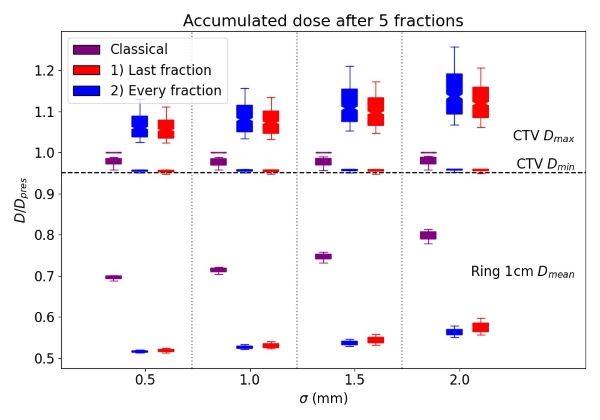
Figure 2: Accumulated dose at the end of all simulated treatments for classical margins and the adaptive strategies.
In figure 1 we show the maximum planned dose (as measure of CTV dose inhomogeneity) for the different strategies. The accumulated effect can be seen in figure 2. We found that the CTV Dmin was reached in all strategies, with an increase of CTV Dmax up to 110-115% in the adaptive strategies. We also found an almost 30% reduction of the mean dose in a 1 cm ring around the CTV.
Conclusion
Abolishing PTV margins for the first N-1 fractions, while correcting for missed dose was feasible. CTV coverage can be ensured at the desired level, at the cost of higher dose inhomogeneity in the CTV, increasing with random uncertainty. While the radiobiology of non-constant dose prescription requires further investigation, the absence of treatment margins in the first N-1 fractions, notwithstanding the higher CTV Dmax, substantially lowers the average normal tissue dose in the first centimetre compared to a classical margin and prescription.