The role of Acuros XB in the inverse optimization of lung VMAT plans evaluated by 4DCT reality
PO-2015
Abstract
The role of Acuros XB in the inverse optimization of lung VMAT plans evaluated by 4DCT reality
Authors: Andrea Bresolin1, Francesco La Fauci1, Giacomo Reggiori1,2, Nicola Lambri1,2, Marco Pelizzoli1, Sara Parabicoli1, Pasqualina Gallo1, Lucia Paganini1, Francesca Lobefalo1, Stefano Tomatis1, Marta Scorsetti1,2, Pietro Mancosu1
1IRCCS Humanitas Research Hospital, Radiotherapy and Radiosurgery Department, Milan, Italy; 2Humanitas University, Department of Biomedical Sciences, Milan, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
AcurosXB (AXB) is a type C algorithm for the delivered dose estimation. AXB for lung VMAT plan optimization could induce higher fluency in the low density inside PTV in comparison to type A/B algorithms. The goals of the current work are: (1) to highlight the role of AXB during the inverse optimization of lung plans (2) to investigate the likely scenario tracking the GTV amongst the 4DCT phases (3) to show the difference between a homogeneous and inhomogeneous dose prescription case.
Material and Methods
Modulated plans for lung hypo-fractionated radiotherapy (48-50Gy in 4-5 fractions) were considered. The free-breathing CT (FBCT) was used for dose optimization and reporting. In all cases, the final dose calculation was performed with AXB. Two optimizations were considered: w/ and w/o intermediate dose with AXB, i.e., Pencil Beam (PB) + AXB algorithms vs. PB alone. Each optimization was performed for both homogeneous (i.e., PTV_V100%=50% with PTV_V95%>95% and PTV_V105%<5%) and inhomogeneous (i.e., PTV_V98%=99% with Internal Target Volume ITV_V120%=99% and 135%<Dmax<140%) dose prescriptions. The four scenarios were calculated with AXB on each 4DCT phase. The plan sum of all 4DCT 10-phases (equally normalized to the total MU) was used as reference for each case. The mean dose (Dmean) difference between PTV in the optimized plans of each scenario and GTV in the corresponding plan sum was evaluated. The entire procedure was conducted using a fully automated tool developed with the Eclipse Scripting API. Specifically, GTV was automatically defined in each 4DCT phase as the volume segmented by a threshold equal to the Mean+StdDev Hounsfield Unit (HU) in the PTV that overlaps the ITV.
Results
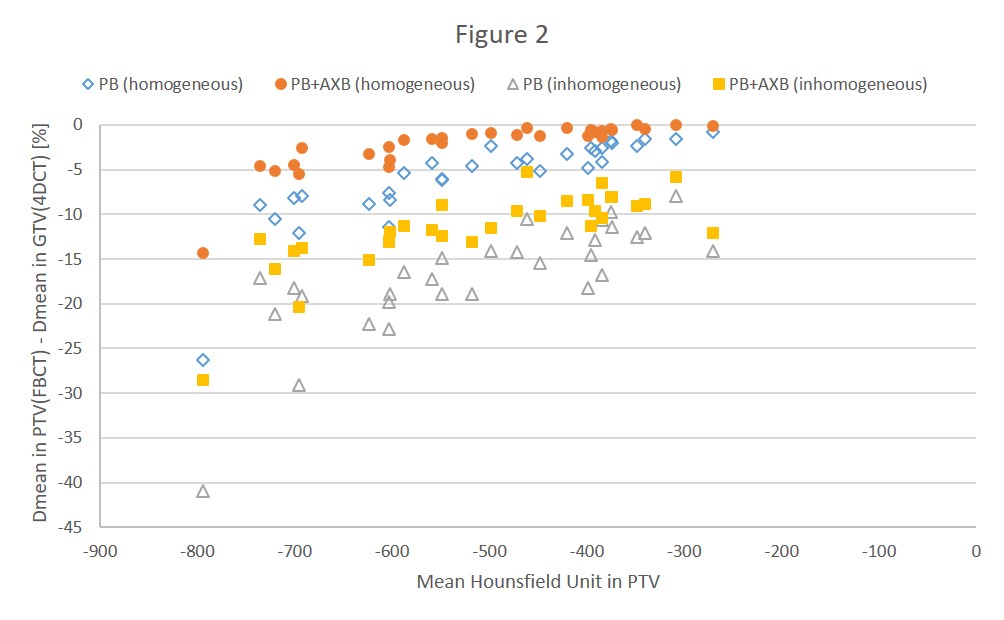
31 lung VMAT cases were analyzed: a total of 124 optimizations and 1240 dose calculations over each 4DCT phase were performed. The range of movement for the GTV centroid detected by 4DCT was between 0.4-4.2mm, 0.3-7.7mm and 0.1-15.3mm in Right-Left, Anterior-Posterior and Inferior-Superior directions respectively. Figure 1 shows the Dmean difference between ITV and the peripheral volume PTV-ITV according to the mean HU in PTV. This difference was similar w/ and w/o intermediate dose in the inhomogeneous prescriptions, while for the homogeneous cases AXB showed a lower Dmean difference than PB. Figure 2 plots the Dmean difference between PTV in the FBCT and GTV in the plan sum for all 4DCT phases. The actual dose to GTV was systematically greater than in PTV with a clear dependence on HU; the AXB dose estimate was very close to the reference in 4DCT for the AXB with homogeneous prescription case when mean HU in PTV was >-500HU.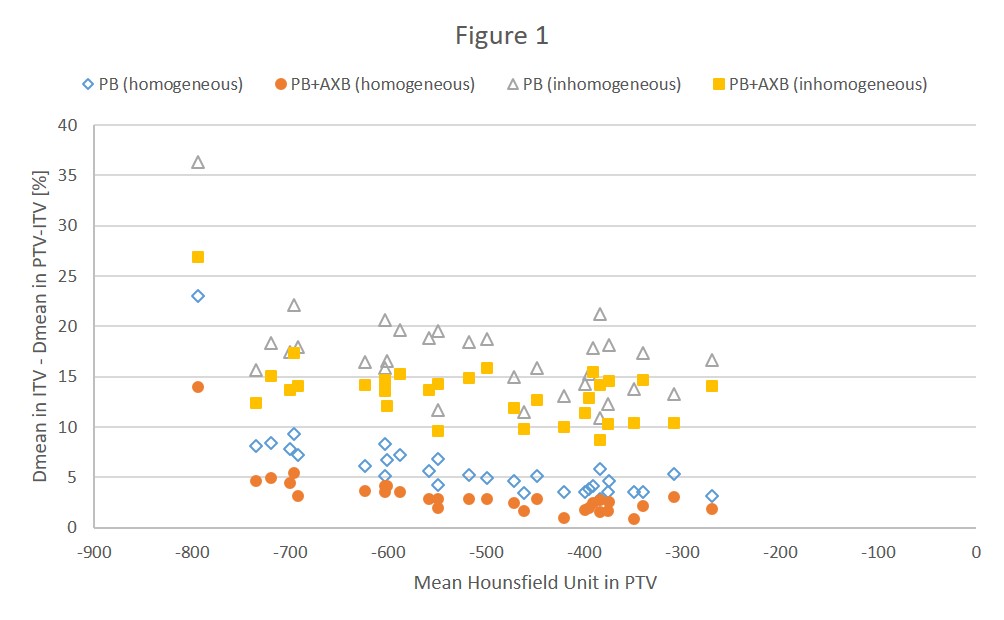
Conclusion
AXB played a role in lung plan optimization when the intermediate dose was applied. The effect was to minimize the dose difference within low density peripheral areas inside PTV. The dose coverage of GTV was ensured both with homogeneous and inhomogeneous dose prescription.