A total of 45 plans were compared for this study. Both in-silico SBRT and delivered IMRT plans were able to create the dose gradient (+10.34%) needed for the SIB prescription and have reached the primary planning goal of D95% > 95% for both PTVs in every plans. However, the comparison of dose coverage objectives established that statistically significant difference exists.
Comparing delivered IMRT vs in-silico SBRT plans with prescription to 85% IDL, showed better coverage of PTV-p and, especially, of PTV-d, where a significant increase of median D95%, D2%, D0.03cc, D50% V100% and V110% was observed respect to delivered plans.
The same difference for PTVs dose coverage, was maintained in a lower degree when comparing the median value of delivered IMRT plans versus in-silico SBRT plans with prescription to 95% IDL.
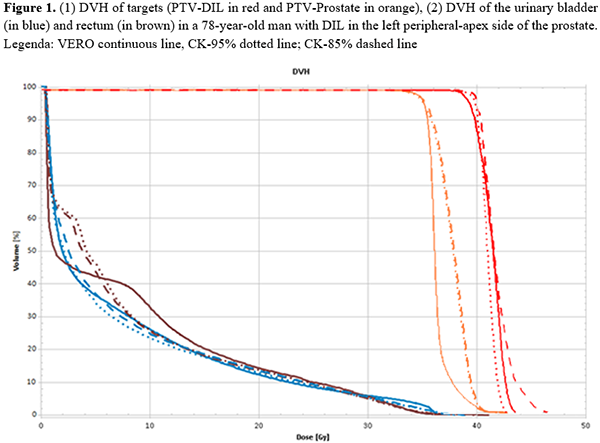
Concerning the organs at risk (OARs), the three techniques maintained the dose distribution well below all the prescribed OARs dose constraints in every plan. Overall, the in-silico SBRT CY plans with prescription to 85% IDL resulted to be the best technique able to reach a maximum dose of 47 Gy to the DIL while respecting all the OARs constraints applied in IMRT-delivered VERO plans. An example of dose distribution of the three tecniques can be found in Figure 1.