Whole brain radiotherapy with hippocampal avoidance using Varian HyperArc: Preliminary study
Miguel Martinez Albaladejo,
Spain
PO-2066
Abstract
Whole brain radiotherapy with hippocampal avoidance using Varian HyperArc: Preliminary study
Authors: Miguel Martinez Albaladejo1, Vicente Puchades Puchades1, Jonathan Suárez Arteaga1, David Ramos Amores1, Alfredo Serna Berná1
1Complejo Hospitalario Universitario de Cartagena-Servicio Murciano de Salud, Servicio de Radiofísica y Protección Radiológica, Cartagena, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
The purpose of this work is to preliminarily evaluate the use of Varian HyperArc (HA) as a planning and treatment strategy for whole brain radiotherapy with hippocampal avoidance (WBRTHA) in the radiotherapy department at the Complejo Hospitalario Universitario de Cartagena (CHUC).
Material and Methods
14 patients treated in Clinacs for WBRTHA by the standard VMAT technique (TP), 4 coplanar 6MV arcs, were retrospectively planned for the TrueBeam HD-MLC linac (TPTB) and using the newly commissioned HA technique (1 full+3 non-coplanar 6FFF arcs, maximum 1400MU/min).
The OAR brain, hippocampi, lenses, optic nerves, and brainstem were contoured on MRI and CT datasets. The median of the PTV, defined as the brain excluding the 3mm expanded region from hippocampi, was prescribed 25 Gy (12 cases) or 30 Gy (2) in 10 fractions.
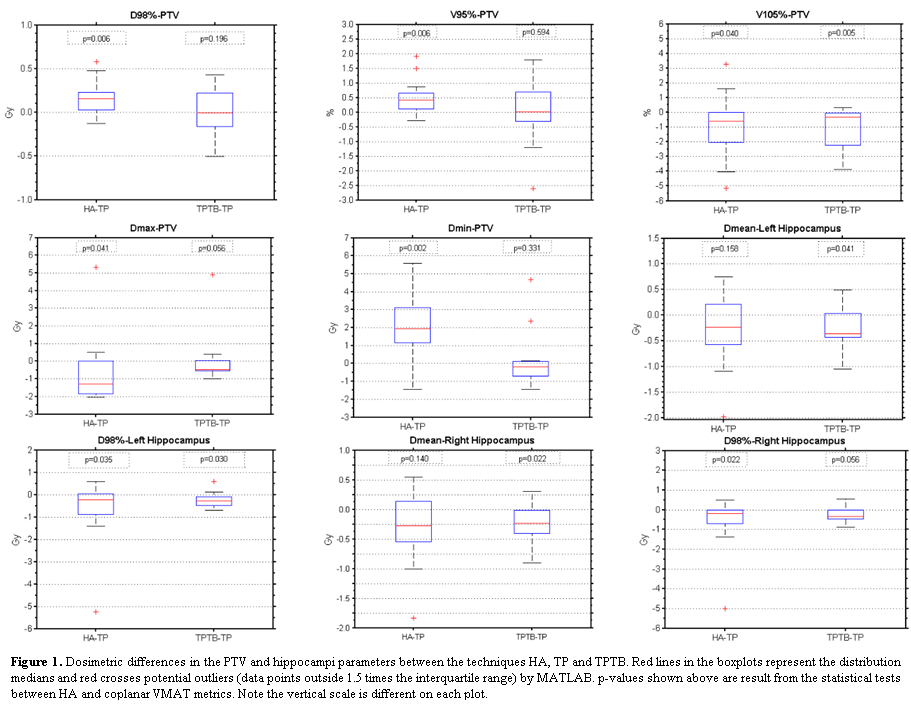
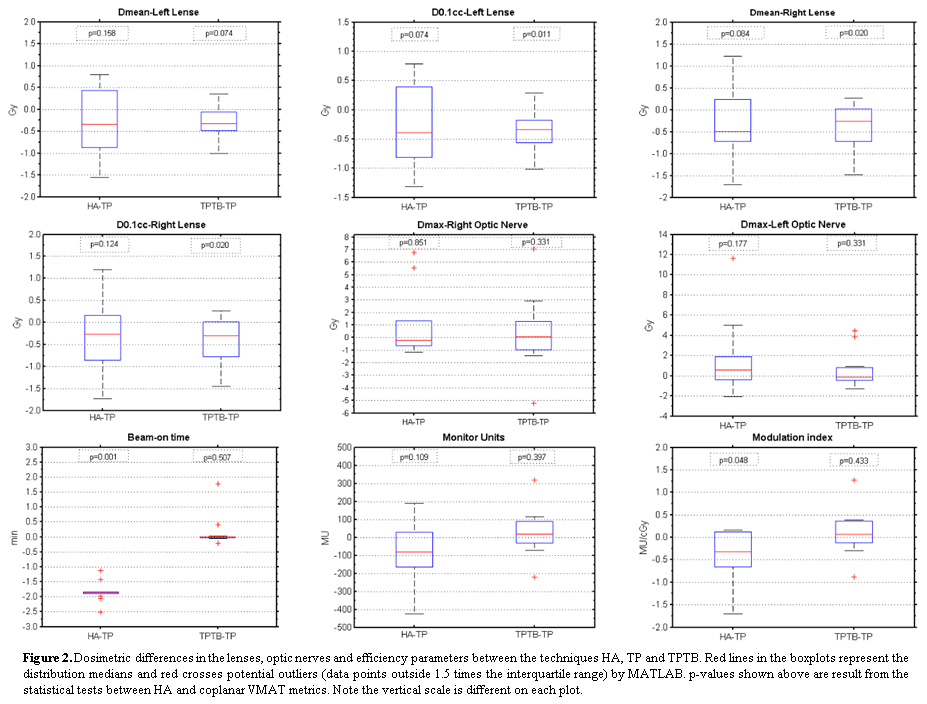
The plans were evaluated using as dosimetric parameters the PTV volume that receives 105% and 95% of the prescribed dose (V105% and V95%), the doses to the 98% (D98%) and 2% (D2%) of the PTV, the maximum (Dmax) and minimum (Dmin) doses to PTV, in addition to the mean doses, the D98% and D0.1cc to the hippocampi and lenses, and finally the Dmax to brainstem and to both optic nerves. Planning time, beam-on time, MUs and modulation index were estimated, and γ-analysis results were also assessed to ensure QA. Statistical significance was performed between HA and TP and between TPTB and TP, using Wilcoxon's signed rank test with a significance level of α=0.05.
Results
All plans satisfied the local dosimetric acceptability criteria. The HA plans demonstrated significant improvements in the PTV dosimetric quality that included a reduction in the parameters V105% (-1.1±2.0%), D2% (-0.2±2.7%), Dmax (-0.6±3.4 Gy) and an increased Dmin of 2.0±4.5 Gy and V95% of 0.5±1.0 %, compared with TP (Figures 1 to 2). A significant decrease in OAR doses was also found for the HA plans, as shown by the reduction in the Dmin to both hippocampi of -0.6±1.3 Gy, in the mean doses to the hippocampi (-0.3±0.8 Gy) and to both lenses (-0.6±0.7 Gy). HA plans resulted in significantly shorter planning and beam-on times with regards to TP (TPTB), on average by 52.4 minutes (26.8) and 1.8 minutes (2.0), respectively. The MUs and modulation index were lower for HA compared with TP (75.4MU and 0.4cGy/MU) and TPTB (105.5MU and 0.5cGy/MU). No significant differences were found between QA results based on γ-metrics.
Conclusion
This first study demonstrates using HA as an efficient strategy for WBRTHA treatments in a TrueBeam HD-MLC linac. As in reference studies, the main advantages found for this modality compared to coplanar VMAT are the gains in the dosimetric OAR sparing, the reduction of the high doses to PTV and the increase of minimum doses to PTV, being less time-consuming (stressed by FFF) and dependent on the user experience. We believe that this increase in efficiency and confidence due to process automation ultimately improves patient care. Therefore, HA has become our new standard technique for WBRTHA.