Separated single arc VMAT with rectangular collimation (SA-VMAT) for prostate SBRT.
PO-2064
Abstract
Separated single arc VMAT with rectangular collimation (SA-VMAT) for prostate SBRT.
Authors: Hisato Nagano1, Hiroko Yokoyama1, Masahiro Kato2, Harumitu Hashimoto1, Takahiro Shimo2, Motoi Watanabe1, Masanori Nakanishi1, Hiroshi Suzuki1, Yuichi Kaneko1, Kazutomo Kobayashi1, Chihiro Takano1, Satoko Tanaka1, Yu Goto1, Erika Horikoshi1, Masafumi Notani1
1Shonan Fujisawa Tokushukai Hospital, Radiation oncology, Fujisawa, Japan; 2Tokyo-West Tokushukai Hospital, Radiation oncology, Akishima, Japan
Show Affiliations
Hide Affiliations
Purpose or Objective
In the cases of the prostate VMAT-SBRT we used multiple arcs (MA-VMAT) for the sake of realizing ideal clinical goals (CGs). As the number of arc increases, the goals may get closer but estimated treatment time (ETT) should increase. We tried separated single arc (gantry angle; 181 - 290, 290 - 70, 70 - 179 degrees) with rectangularly (5, 95, 5 degrees) collimated VMAT (SA-VMAT), and reported time saving ability of this method under the same CGs used for the MA-VMAT.
Material and Methods
From June 2022, thirty five patients were retrospectively selected from our database. Median of age was 77 (range 55 - 86) years. High, intermediate and low risks were distributed as 26, 7 and 2, respectively. Initial PSA value was ranged from 4.014 to 339.0 (median 9.862) ng/ml. GS was 4 to 9 and median value was 8. Numbers of patients diagnosed as T1, T2 and T3 were 5, 20 and 10, respectively. Median volume of prostate was 27.8 (range 13.08 - 82.55) ml. These 35 MA-VMAT plans were recalculated by SA-VMAT using the same CGs with some modifications of constrains. Values of CGs and ETT were compared and estimated by paired t-test. Dose calculation was done using RayStation 10. CRAN R and Rstudio used for statistical calculation.
Results
In MA-VMAT, ETT increased about 80 sec per arc ([number of arc; ETT sec], 2; 252, 3: 328, 4; 409, 5; 450, 6; 617). Details of CGs and achieved values calculated by SA or MA are presented in Table with p-values of t-test.
Structure
| Goal
| SA
| MA
| p-Value
|
Bladder
| V37Gy < 5 ml
| 2.96
| 2.75
| 0.342
|
Bowel
| D1ml < 30 Gy
| 19.10
| 17.17
| 0.001
|
Femoral head_Lt
| Max < 27.5 Gy
| 15.37
| 11.73
| 0.000
|
Femoral head_Rt
| Max < 27.5 Gy
| 16.89
| 11.83
| 0.000
|
Neural Band
| D50% < 40 Gy
| 38.46
| 37.92
| 0.001
|
penile bulb
| D0.1ml < 29.5 Gy
| 15.95
| 11.59
| 0.000
|
Prostate
| V40Gy > 90 %
| 94.49
| 96.75
| 0.004
|
PTV
| Conform(35 Gy)
| 0.67
| 0.78
| 0.000
|
| V29Gy > 99.9 %
| 100.00
| 100.00
| 1.000
|
| V36.25Gy > 95 %
| 96.00
| 95.88
| 0.346
|
Rectum
| D20% < 44 Gy
| 10.28
| 10.26
| 0.885
|
| D40% < 20 Gy
| 6.19
| 6.45
| 0.052
|
| V36Gy < 2 ml
| 1.72
| 1.63
| 0.093
|
Skin
| Max < 30 Gy
| 16.76
| 14.61
| 0.000
|
Testes
| Max < 2 Gy
| 0.58
| 0.54
| 0.010
|
Urethra
| D20% < 44 Gy
| 40.63
| 40.26
| 0.009
|
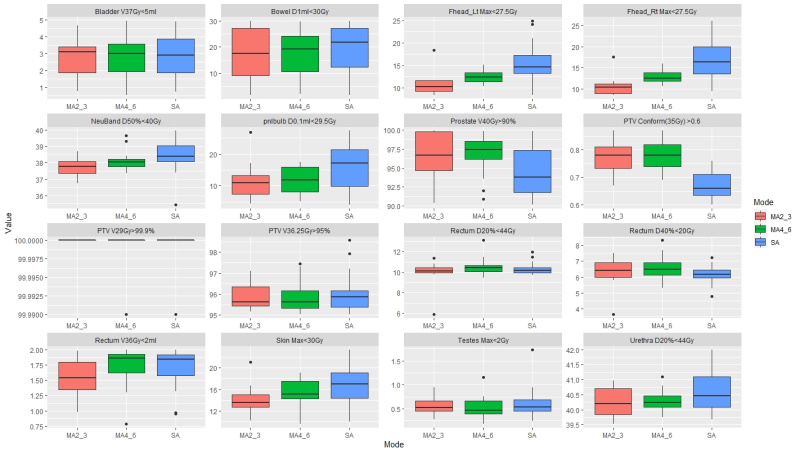
Box-plots of values of CGs were presented in Figure. Average ETT of SA (258 sec) and MA (369 sec) were statistically different (p < 0.0001). SA satisfied all CGs as MA had done. Critical structures such as rectum, bladder and PTV had statistically similar mean values. CGs of those structures which were not strictly restricted had better values in MA compared to SA, however 4 to 6 arcs plan not always had better values compared to 2 or 3 arcs plan.
ETTs of SA were decreased from that's of MA 28.5% in average (range 2.6 - 54.7 %). Averages of EET grouped by arc were decreased to that of SA by 9, 26, 32, 40 and 54% as numbers of arc increased from 2 to 6.
Conclusion
SA-VMAT had sufficient ability to treat prostate cancer in our CG perspective compared to MA-VMAT. It also had time (and energy) sparing feature. On average 28% of ETT had decreased. As number of arc increased, ETT increased. SA-VMAT may be a sustainable and good clinical solution.