CyberKnife with InCise MLC versus VMAT with FFF in SBRT for Prostate cancer: A dosimetric comparison
Wisawa Phongprapun,
Thailand
PO-2045
Abstract
CyberKnife with InCise MLC versus VMAT with FFF in SBRT for Prostate cancer: A dosimetric comparison
Authors: Wisawa Phongprapun1, Putthipong Chanwichu1, Wiwatchai Sittiwong1, Shoulakin Kunchitshoulakul1, Pittaya Dankulchai1
1Siriraj Hospital, Radiation oncology, Bangkok, Thailand
Show Affiliations
Hide Affiliations
Purpose or Objective
Prostate cancer is one of the most common cancers in men. Stereotactic body radiation therapy (SBRT) is a technique to deliver high doses with high accuracy and precision in a few fractions. Cyberknife (CK) is one option of radiotherapy machine that is capable of delivering SBRT for prostate cancer; however, the cost per unit is relatively high and the availability of CK was limited in a few radiotherapy centers. Volumetric Modulated Arc Therapy (VMAT) technique to deliver SBRT plan was an appealing alternative option to SBRT delivered by CK. The objective of this study is the dosimetric comparison between CK-SBRT and VMAT-SBRT treatment in prostate cancer
Material and Methods
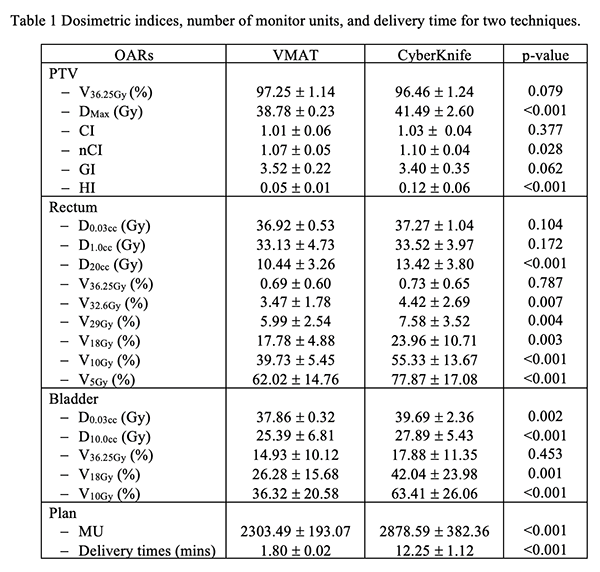
Twenty prostate cancer patients treated by CK M6 were selected and replanned using VMAT. Dose prescription to prostate was 36.25 Gy in 5 fractions. For the CK, plans were generated by Incise MLC instead of fixed or Iris cone to reduce the treatment time. For VMAT, plans were generated for TrueBeam STx with the 'high definition' 120‐leaf multileaf collimator(HD120-MLC) and used two partial arcs (200-160 clockwise arcs with collimator angle15 and 160-200 counterclockwise arcs with collimator angle345) with a flattening-filter-free 10MV photons. Moreover, volume of PTV receiving 95% of the prescription dose in VMAT plans was normalized to be similar to the CK plans. Dose indices related to target coverage, dose-volume histogram parameters for the target and organs at risk(OAR), as well as Conformity index(CI) and new Conformity index(nCI), Gradient index(GI), and Homogeneity index(HI) were compared. The number of monitor units (MU) and the estimated treatment delivery times of each plan were also reported.
Results
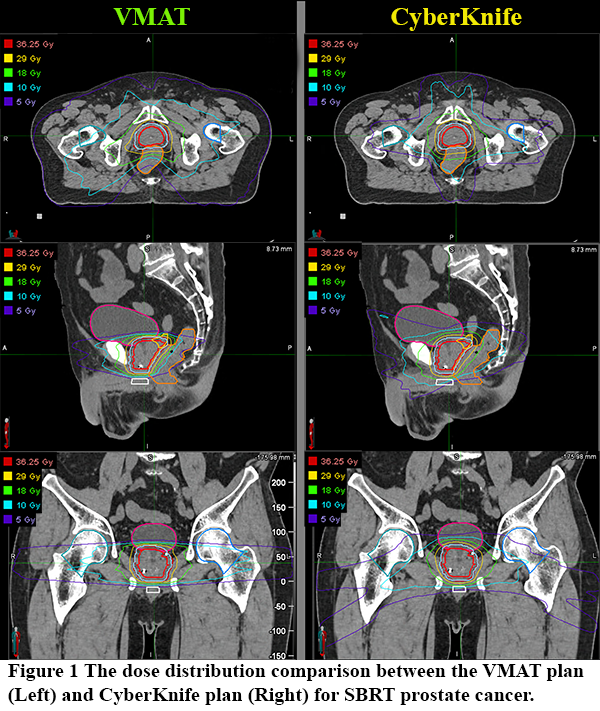
The dose distribution of two techniques was shown in Figure 1. The volume of PTV received 36.25 Gy for VMAT was higher than CK (VMAT:97.25 1.14%, CK:96.46 1.24%) but did not reach statistically significant(p=0.079). The doses conformed to PTV of VMAT were better than CK with statistically significant in nCI (VMAT: CI1.01 0.06 and nCI1.07 0.05, CK: CI1.03 0.04 and nCI1.10 0.04, p=0.377 and 0.028 respectively); however, the dose rapid falloff of CK-SBRT was not statistically differenced VMAT-SBRT (CK: GI3.40 0.35, VMAT: GI3.52 0.22, p=0.062). The dose homogeneity of VMAT-SBRT was higher than CK (VMAT: HI0.05 0.01, CK: HI0.12 0.06, p<0.001). In terms of OARs sparing, VMAT was reduced dose to OARs greater than CK, as shown in Table 1. Nevertheless, VMAT provides the number of MU and treatment delivery times less than CK (VMAT: MU2303.49 193.07 and delivery time1.80 0.02 mins, CK: MU2878.59 382.36 and delivery time12.25 1.12 mins, p<0.001)
Conclusion
VMAT-SBRT is able to deliver a conformal plan for treating SBRT in prostate cancer which can be an alternative option to CK-SBRT. However, image-guided radiotherapy with fiducial markers should be careful in delivering SBRT in prostate cancer, especially for VMAT-SBRT.