SBRT AS A RADICAL LOCAL TREATMENT IN OLIGOMETASTATIC DISEASE
Macarena M. Teja Ubach,
Spain
PO-1610
Abstract
SBRT AS A RADICAL LOCAL TREATMENT IN OLIGOMETASTATIC DISEASE
Authors: Elisabet Gonzalez Del Portillo1, Ana Castaño Cantos2, Rafael Rosel Aller3, Marta Rodríguez Roldán4, Isabel Garrido Botella5, Macarena Teja Ubach4, Mercedes González Cantero4, Beatriz Debén Méndez4, Víctor Duque Santana4, Isabel Rodríguez Rodríguez4, Luis Alberto Glaría Enríquez4, Ane Escribano Uzcudun4, Belén Belinchón Olmeda4, Áurea Manso de Lema4, Raúl Matute Martín4, Lara Miralles Olivar4, Rosa María Morera López4
1HOSPITAL UNIVERSITARIO LA PAZ, RADIATION ONOLOGY , MADRID, Spain; 2Hospital Universitairo La Paz, Radiation Oncology, Madrid, Spain; 3Hospital Universitario La Paz, Radiationn Oncology, Madrid, Spain; 4Hospital Universitario La Paz, Radiation Oncology, Madrid, Spain; 5Hospital Universitario La Paz, Radiation Oncology , Madrid, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
Oligometastatic patients benefit from radical local treatment, including SBRT (stereotactic body radiation therapy). The selection criteria for these patients are not well established in the literature, but it is generally accepted that a patient with up to 5 metastases is an oligometastatic patient. The latest publications classify these lesions according to whether they are genuine vs. induced, de novo vs. repeat, synchronous vs. metachronous, oligorecurrence vs. oligopersistence vs. oligoprogression, with the aim of better classifying these lesions and patients in order to offer the best therapeutic strategy.
The aim of this work is to analyze the diagnostic criteria for the oligometastatic disease and the results of SBRT in our centre. These results will be the first step in determining which types and subtypes of patients and lesions benefit most from this therapeutic strategy.
Material and Methods
Patients who received SBRT treatment from January to December 2020 were included. The primary tumour could be any location. The location of the lesion treated with SBRT was extracerebral. Fractionation schedules ranged from 1 to 8 fractions depending on location and patient characteristics.
Results
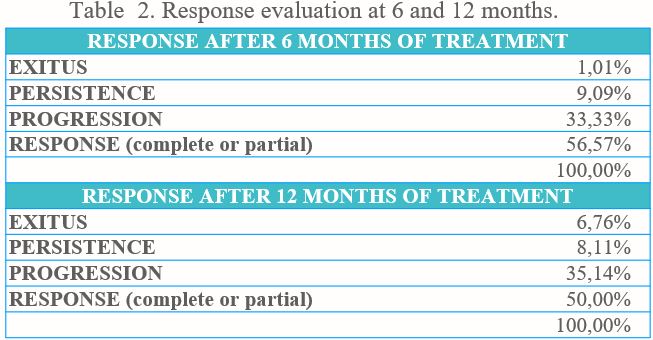
Seventy-seven patients and 103 lesions were treated by SBRT. The most frequent primary tumor and histology were prostate cancer (40.26%) and adenocarcinoma (70.13%), respectively. The 80.52% of patients were classified as oligometastatic (<5 lesions), and 87.01% corresponded to 'genuine oligometastatic disease'. In this group, the majority were 'de-novo oligometastatic disease'(79.22%). These patients were metachronous in 66.23%. Oligorecurrence occurred in 44.16%, oligoprogression in 33.77% and oligopersistence in 14.29% of patients at diagnosis of the metastasis to be treated. Table 1 describes the schedules used. The most frequent were 30 Gy in 3 fractions (36.89%) and 60 Gy in 3-5 fractions. The most frequent locations were bone (38.24%), lung (25.49%) and ganglion (20.59%). The evaluation at 6 and 12 months showed a complete or partial response in 56.57% and 50%, respectively (Table 2).
Only 7 patients developed grade 1 acute toxicity and only one patient developed grade 1 chronic toxicity. 18.18% were exited during the first year of evolution.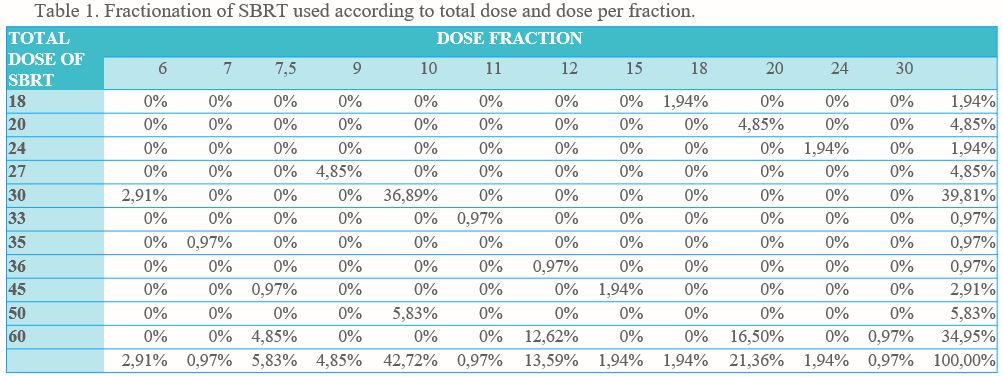
Conclusion
SBRT offers a radical local treatment in selected patients. It is essential to standardize selection criteria of oligometastatis disease for an adequate indication of SBRT. More studies are needed, we are analysing more cases.