Value of a systematic cardiac workup by a cardiologist for prostate cancer patients treated with ADT
PO-1478
Abstract
Value of a systematic cardiac workup by a cardiologist for prostate cancer patients treated with ADT
Authors: Maximilien Rogé1, Valentine Guimas2, Stéphane Supiot2, Elvire Martin Mervoyer3
1Centre Henri Becquerel, Department of radiation Oncology, Rouen, France; 2Institut de Cancérologie de l'Ouest, Department of Radiation Oncology, Nantes, France; 3Institut de Cancérologie de l'Ouest, Department of cardio-oncology, Nantes, France
Show Affiliations
Hide Affiliations
Purpose or Objective
Androgen deprivation therapy (ADT) increases cardiovascular risks. Prevention is the cornerstone of cardiac management, but there is currently no consensus regarding the initial cardiac workup to be performed or when to refer the patient to a cardiologist.
Our study aimed to report the cardiac findings of consecutive patients with prostate cancer (PCa) requiring ADT who underwent systematic cardiac workups by a cardiologist.
Material and Methods
This retrospective monocentric included consecutive patients with PCa who had completed a cardiac workup (CW) in the cardio-oncology department between January 2019 and August 2022. Baseline CW, before the initiation of ADT or within the first 90 days, included a physical exam, transthoracic echography and electrocardiogram. The primary objective was to determine the number of new diagnoses of coronary artery disease (CAD). Secondary objectives included the number of other cardiac diseases and the number of introductions/changes in cardiovascular treatment.
Results
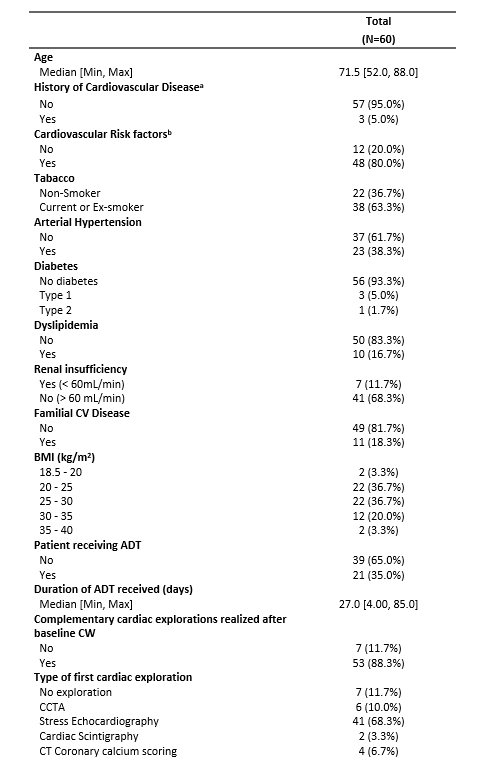
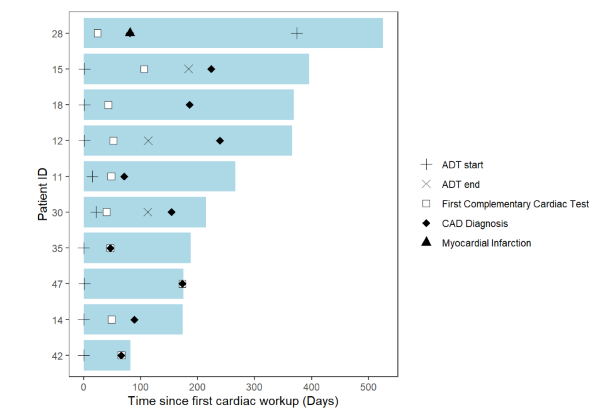
Sixty patients were included in our study. Characteristics of patients at the baseline CW are available in table 1. After a median follow-up of 9 months (1–36), 10 CAD were diagnosed (16.7%). The median time to diagnose CAD was 122 days (47–339) (swimmerplot). Of the 50 patients without a diagnosis of CAD, 22 (44.0%) underwent therapeutic intervention by the cardiologist. One patient was diagnosed with atrial fibrillation requiring treatment (Beta-blockers and anticoagulation). One diabetic patient had a diagnosis of microcirculation disorder that required beta blockers. One was diagnosed with a conductive disorder requiring a pacemaker. One was diagnosed with a severe obstructive sleep apnea syndrome requiring continuous positive airway pressure, and 18 other patients had an introduction or modification of medical treatment for cardiovascular risk factors (hypertension and/or dyslipidemia). No patients died of cardiac causes during follow-up. Of the 60 patients who underwent systematic cardiac workups, 32 (53.3%) had a therapeutic intervention after this evaluation.
Conclusion
Cardiac and coronary assessment in prostate cancer patients treated with ADT is a relevant strategy leading to therapeutic intervention in half of the patients. Nevertheless, it is necessary to develop prospective tools to better select patients who will benefit from this CW.