Intrafractional prostate movements and toxicity in a randomized trial with small-margin radiotherapy
Johan Staby Olsén,
Sweden
PO-1515
Abstract
Intrafractional prostate movements and toxicity in a randomized trial with small-margin radiotherapy
Authors: Johan Staby Olsén1
1Örebro University, Oncology, Örebro, Sweden
Show Affiliations
Hide Affiliations
Purpose or Objective
Moderately hypofractionated radiotherapy (RT) with high dose-rate brachytherapy as boost is considered a suitable treatment option in patients with localized prostate cancer. Hypofractionated RT requires high accuracy in dose delivery to enable reduced treatment margins to minimize the dose to organs at risk. Real-time monitoring of intrafractional prostate movements could theoretically enable higher precision in dose delivery and smaller margins.
The present study aimed to investigate whether smaller margins could enable an accelerated delivery of hypofractionated RT (five times vs. three time per week) without increased toxicity. The study also aimed to assess the pattern of intrafractional prostate movements using a high-precision real-time tracking system.
Material and Methods
During 2017 to 2020, 34 prostate cancer patients, planned for combined high dose rate brachytherapy (14,5 Gy x 1) and external beam RT (3 Gy x 14) were included in a randomized trial to receive treatment either three or five times per week. External RT was delivered utilizing small margins (3 mm) using the Raypilot system for real-time tracking of intrafractional prostate movements. Movements were continuously monitored in three dimensions during a total of 399 fractions. The beam was turned off if a displacement exceeded 2 mm for more than four seconds and patients were repositioned if the displacement persisted for 30 seconds. Toxicity was primarily assessed using patient-reported outcome measures through EORTC QLQ-C30 and QLQ-PR25.
Results
In total, 34 patients (17 in each study arm) were included in the study (median age was 70 years).
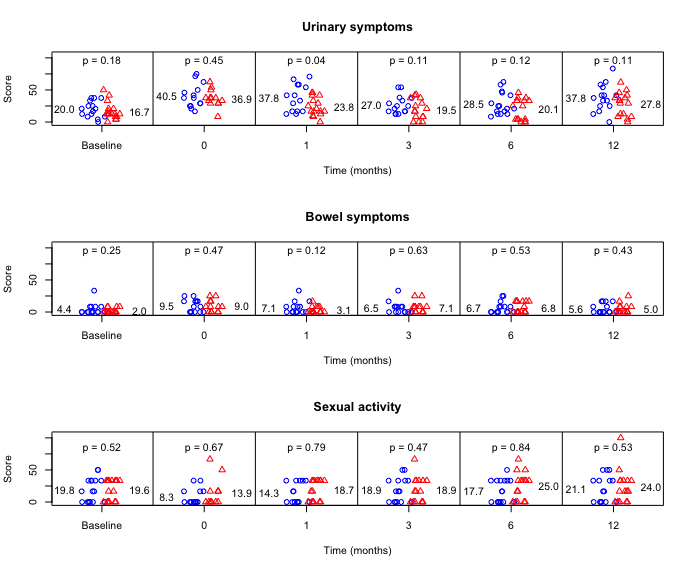
For the entire study cohort, the average urinary symptoms score increased from 18.2 to 32.6 (p = 0.003) and the average global health status score decreased from 79.2 to 67.5 (p = 0.04) during the first 12 months of follow-up. No statistically significant long-term differences in toxicity between the two delivery schemes were observed (Fig 1).
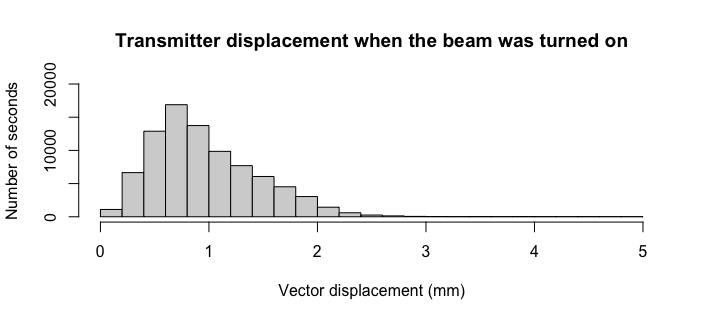
Transmitter displacement was less than 2 mm during 97.0% of the time and less than 3 mm during 99.9% of the time (Fig 2). A displacement exceeding 2 mm in any dimension for at least 4 seconds was seen in 42 (11 %) fractions. The most common event was a negative vertical displacement (transmitter displaced towards the back of the patient). Patients having the transmitter located near the base of the prostate, had no treatment interruptions. Patients who had the transmitter placed centrally or near the apex had an average of 2.9 and 1.5 treatment interruptions per fraction, respectively.
Conclusion
Small margins when using a real-time tracking system are feasible and might facilitate more frequent dose delivery schemes. Provided that the CTV is properly delineated, and the transmitter approximately centrally located, a 3 mm margin can be considered safe when using a real-time tracking system with only a limited part of the radiation to be delivered when the target is displaced more than 2 mm.