The Feasibility of SGRT on Locally Advanced Cervical Cancer Patients with Bladder Protocol
PO-1840
Abstract
The Feasibility of SGRT on Locally Advanced Cervical Cancer Patients with Bladder Protocol
Authors: qiong liu1, Lin Su1, Du Tang1, Zhifo Wu1, Zhen Yang1, Hua Peng1
1Xiangya Hospital, Central South University, Department of Radiation Oncology, Changsha, Hunan, China
Show Affiliations
Hide Affiliations
Purpose or Objective
The use of SGRT on pelvis region has been a controversial discussion for the past few years. Bladder
inconsistency and topography of pelvis region could be the root cause of the uncertainties including
accuracy and reproducibility. Hence, we would like to study further if a good bladder management
could improve the use of SGRT on cervical cancer patients.
Material and Methods
11 locally advanced cervical cancer patients who received concurrent chemoradiotherapy were enrolled
and analyzed in this study. All patients were positioned in supine position. Patient’s bladder volume
was measured with AvantSonic Z5 Bladder Scanner (AvantSonic Technology Co., Ltd) before
treatment. The difference between the measured bladder volume and CT-sim bladder volume should be
within ±15%. Then, patient was positioned based on isocenter skin markings (1 anterior and 2 laterals).
The couch vertical value was kept the same as the latest CBCT couch acquired value. CBCT was taken
and registration was performed accordingly. 3D translational and rotational shifts were recorded and
applied. Next, SGRT system (OSMS, Varian, Palo Alto, CA) was activated to start monitoring. A
standard recommended region of interest (ROI) was used across all patients, as shown in Figure 1. The
6DoF deltas shown on the SGRT system were recorded. The deltas represented the discrepancies
between CBCT and the reconstructed 3D surface. The average, standard deviation and the error distributions were analyzed using ANOVA test and chi-square test with SPSS software (IBM corp.). A
difference of P < 0.05 was considered statistically significant.
Figure 1: Pelvis ROI

Results
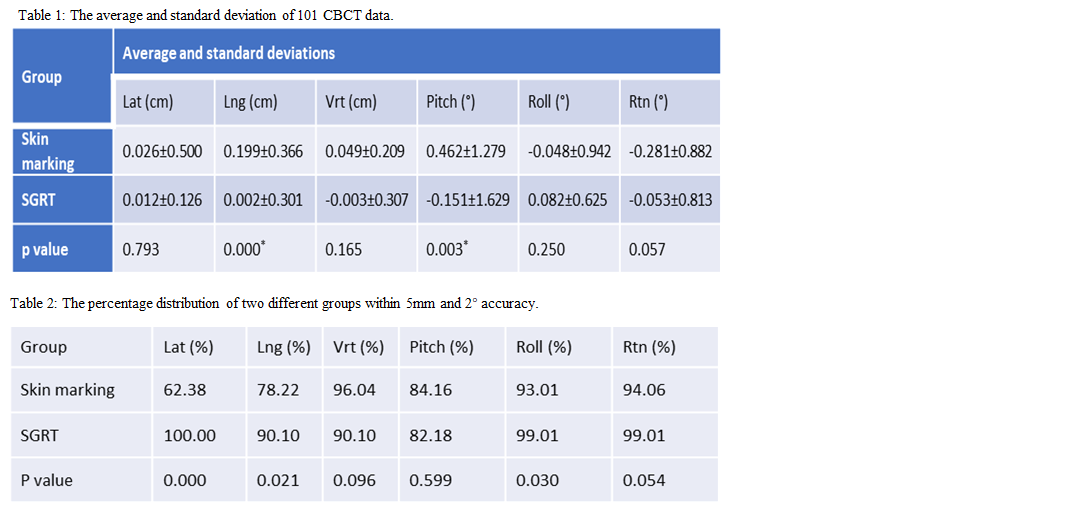
A total of 101 CBCT images were analyzed. The average and standard deviations (Table 1) between
skin marking-based and SGRT-based group were 0.026±0.500cm, 0.199±0.366cm, 0.049±0.209cm and
0.012±0.126cm, 0.002±0.301cm, -0.003±0.307cm in x(lateral), y(longitudinal) and z(vertical)
translational directions; 0.462±1.279°,-0.048±0.942°, -0.281±0.882°, and -0.151±1.629°, 0.082±0.625°,
-0.053±0.813° in Rx(pitch), Ry(roll), and Rz(rotation) rotational direction. The results showed that the
setup error in longitudinal and pitch could be improved with SGRT system. The percentage of
positioning accuracy within 5mm and 2° were shown in Table 2. The positioning accuracy based on
SGRT was comparable to skin marking-based, and SGRT was notably beneficial in lateral, longitudinal and roll direction.
Conclusion
Incorporating a good bladder management can improve the accuracy of SGRT application on cervical
cancer radiotherapy patients. It is feasible, reliable, and potentially mark-free. We will continue to study
for bigger sample size for more concrete conclusion.