Dosimetric comparison between helical tomotherapy and VMAT for pediatric total lymphoid irradiation
PO-1733
Abstract
Dosimetric comparison between helical tomotherapy and VMAT for pediatric total lymphoid irradiation
Authors: Carlos Ferrer1, Concepción Huertas1, Abrahams Ocanto2, David García3, Anne Escribano2, Moisés Sáez1
1HU La Paz, Medical Physics, Madrid, Spain; 2HU La Paz, Radiation Oncology, Madrid, Spain; 3HU La Paz, Medicla Physics, Madrid, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
The aim of this study is to compare the planning of
volumetric modulated arc therapy (VMAT) treatments with those planned with
helical tomotherapy (HT) in pediatric total lymphoid irradiation (TLI).
Material and Methods
TLI treatments are used in the management of
pediatric allogeneic hematopoietic stem cell transplantation (HSCT). TLI
treatment was prescribed to 8 Gy in 4 fractions, and planned on an Elekta
Infinity accelerator with a 160-leaf Agility collimator and VMAT technique with
Elekta Monaco TPS (v. 5.11.02). The same treatment was planned on a HD helical
Tomotherapy, and Accuray Precision TPS. Both linacs have 6 MV nominal energy.
For organs at risk (OAR), in the treatment planned with Monaco, a single cost
function named conformality was used to conform the dose, whereas in the
treatment planned with tomotherapy, multiple auxiliary volumes were created and
several cost functions were used for each one of them, which makes this
planning more complex. The dose objective is that 100% of the PTV is covered by
at least 95% of the prescribed dose. Conformality (CI) and homogeneity (HI) indices
are compared between HT and VMAT, as well as doses to OAR.
Results
The PTV coverage
requirement was met for both treatment planning systems (V100% ≥ 95%), being
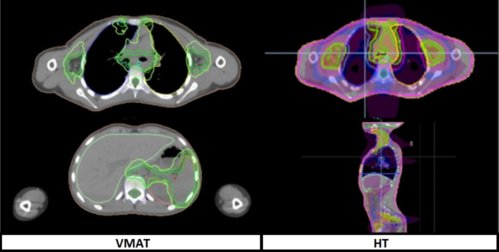
slightly higher for VMAT, 96.6% (VMAT) vs 95% (HT). The treatment planned in HT
presents better CI (1.05 (HT) vs 1.34 (VMAT)) and the dose slightly more
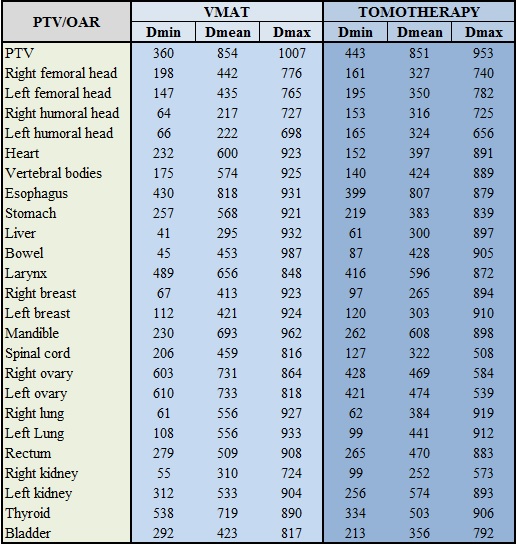
homogeneous (HI= 0.09 (TH) vs 0.14 (VMAT)). The doses to OARs, shown in the
table (in cGy), were similar for both planning systems. Treatment time was
significantly longer in HT, 20.2 min (TH) vs 13.7 min (VMAT).
Conclusion
Planning with HT showed better dose distribution
conformity and homogeneity compared to planning with VMAT. HT planning was
superior in terms of reduction of mean and maximum doses in practically all the
OAR. However, the differences between both are small, with the mean dose in
some OARs slightly lower with VMAT, such as in the left kidney. Longer
treatment time in HT could increase uncertainty due to intrafraction motion.