Advantages of low tesla MR-Linac advanced cost function for online adaptive dose optimization
PO-1732
Abstract
Advantages of low tesla MR-Linac advanced cost function for online adaptive dose optimization
Authors: Lorenzo Placidi1, Matteo Nardini2, Roberto Moretti1, Amedeo Capotosti1, Davide Cusumano1, Luca Boldrini1, Maria Antonietta Gambacorta1, Vincenzo Valentini1, Luca Indovina1
1Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Radiation Oncology, Rome, Italy; 2 Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Radiation Oncology, Rome, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Magnetic resonance guided radiotherapy (MRgRT) allows online dose adaptation based on the daily patient anatomy variation. Treatment planning approach has to be thought to maximise the advantages of online MRgRT, both in terms of dose conformality, treatment time and flexibility to easily adapt the dose distribution to the daily anatomy. The advanced cost function (ACF) for online adaptive dose optimization available in the low tesla MRI-Linac treatment planning system has been evaluated to further boost the advantages of the MRgRT.
Material and Methods
The last eleven treatment plans delivered in our MRI-Linac system have been optimized employing both the simple cost function (SCF) (employed till now for the dose optimization) and the ACF.
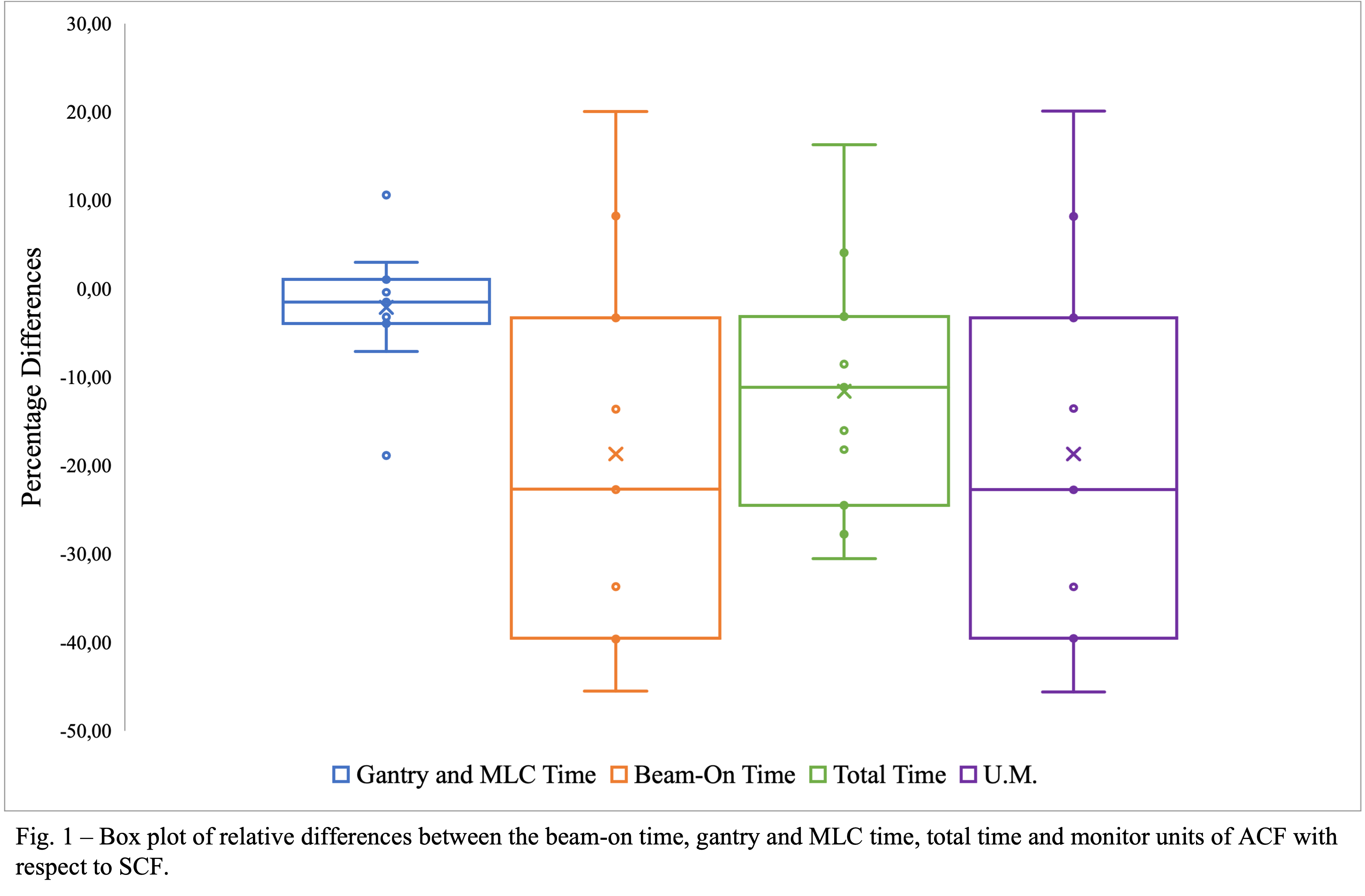
To the difference of SCF, ACF allows the possibility to set multiple penalties for the same structure. Additionally, user can avoid of specifying the structures which are considered as targets: instead, this is determined by those structures that have increased the dose constraints. Additionally, a new approach of online adaptive treatment plan (fewer dummy structures and more generalize workflow) has been implemented to better optimize the process. Patients’ cohort was composed by eleven SBRT treatments (five fractions) located in abdomen (3), thorax (4) and pelvis (4). Planning (treatment time - respectively divided in gantry and MLC, beam on and total time - monitor units (M.U.), number of dummy structures, number of online adaptive optimization) and dosimetric (target (PTV) coverage and OARs constraints based on our institutional guideline) parameters have been compared between dose distribution obtained with the SCF and ACF for dose optimization.
Results
All treatment plans generated employing the ACF have been approved by radiation oncologists and clinically delivered. Results of planning parameters are summarized in figure 1.
An average number of three dummy structures for offline and online dose optimization has been not employed using the ACF approach. Additionally, during the online adaptive process, no more than one dose optimization iteration has been used for the ACF approach. Figure 2 describes the dosimetric comparison for OARs grouped by thorax and abdomen district in terms of minimum, maximum and mean values, as well as for target coverage.
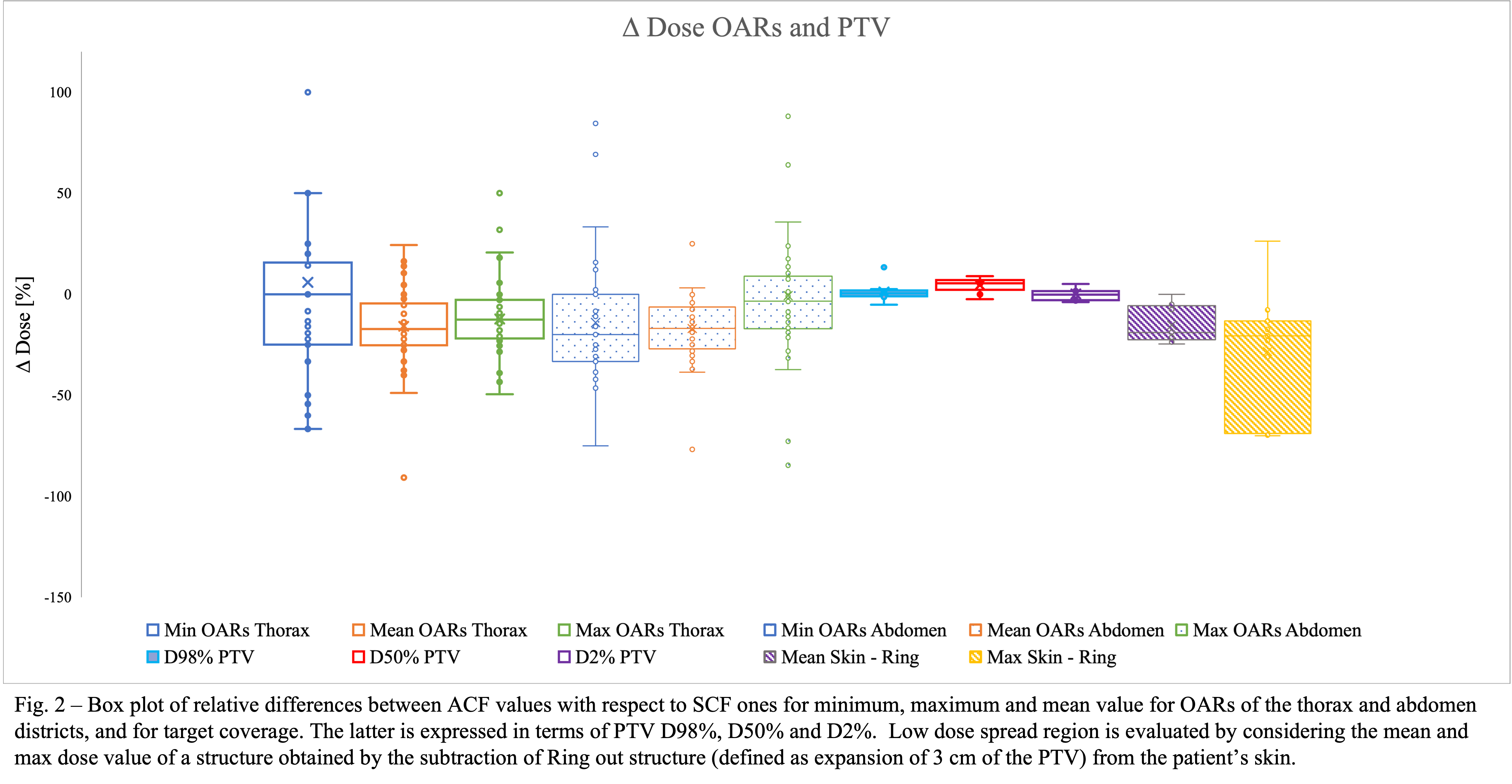
In average, higher OARs sparing and target coverage (especially PTV D50%) have been observed for ACF approach. Also low dose spread region, both in terms of maximum and mean dose, has been reduced by the ACF approach.
Conclusion
Dosimetric and planning advantages have been observed and quantified when ACF approach has been employed. ACF approach reduces the number of Monitor Units used, so allowing an average reduction of the beam on time. Further analysis will be performed in the next future to better quantify how ACF approach improve not only the plan quality but also reduce the time of the online adaptive MRgRT workflow.