Dosimetric evaluation of 6-DOF intra-fraction motion for SGRT of breast cancer patients
Tim-Oliver Sauer,
Germany
PO-1721
Abstract
Dosimetric evaluation of 6-DOF intra-fraction motion for SGRT of breast cancer patients
Authors: Tim-Oliver Sauer1, Oliver Ott1, Christoph Bert1
1Universitätsklinikum Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg, Department of Radiation Oncology, Erlangen, Germany
Show Affiliations
Hide Affiliations
Purpose or Objective
In
this study, the dosimetric effects of intrafractional motion during the
treatment of breast cancer patients, as evaluated by surface guided radiation
therapy (SGRT), is analysed. On a side, the possibility of assessing the
delivered dose patient- and fraction wise was explored; on the other side, suitable
SGRT monitoring threshold values were determined with a treatment plan
robustness analysis on the basis of dose coverage constraints.
Material and Methods
22
patients were treated on two C-arm linacs equipped with an SGRT system. After
positioning using either SGRT only or additional CBCT scans, intrafractional
motion during treatment was recorded using the surface scanner and was analysed
statistically. Dose calculations were carried out with the original treatment
planning system for different 6-DOF shifts, mimicking rigid patient motion. The
dosimetric effect of the observed intrafractional motion was calculated and
evaluated with respect to target coverage and OAR dose. The effect of fixed,
pre-set shifts (1 mm / 1 ° steps) was analysed systematically and maximum shift
values were determined using dosimetric thresholds (minimum relative dose
coverage of 95 %) in order to obtain suitable SGRT monitoring threshold values
for application during treatment.
Results
The
analysis of the effect of pre-set shifts partly showed large deviations from the
originally planned PTV dose coverage (V95% of prescribed dose). A pronounced
asymmetry for vertical translations was observed (see figure 1). The maximum
shift values (based on mean ±
standard deviation) are marked by red arrows in figure 1; for example, for
vertical translations we obtained maximum values of -5 mm (positioned too
high) and +2 mm (positioned to low), respectively. For DIBH patients, the
SGRT based intrafraction motion showed bell-shaped relative frequency distributions
with standard deviations of approximately 1 mm and 1 °, respectively, centered
around zero. Only for vertical translations, the distribution was shifted
slightly towards positive values. The dosimetric effects of intrafractional
motion of the observed shifts were comparable to partial volume effects
stemming from resampling of the dose distribution, which is necessary for dose
summation of different scenarios; details thereof are currently under
investigation.
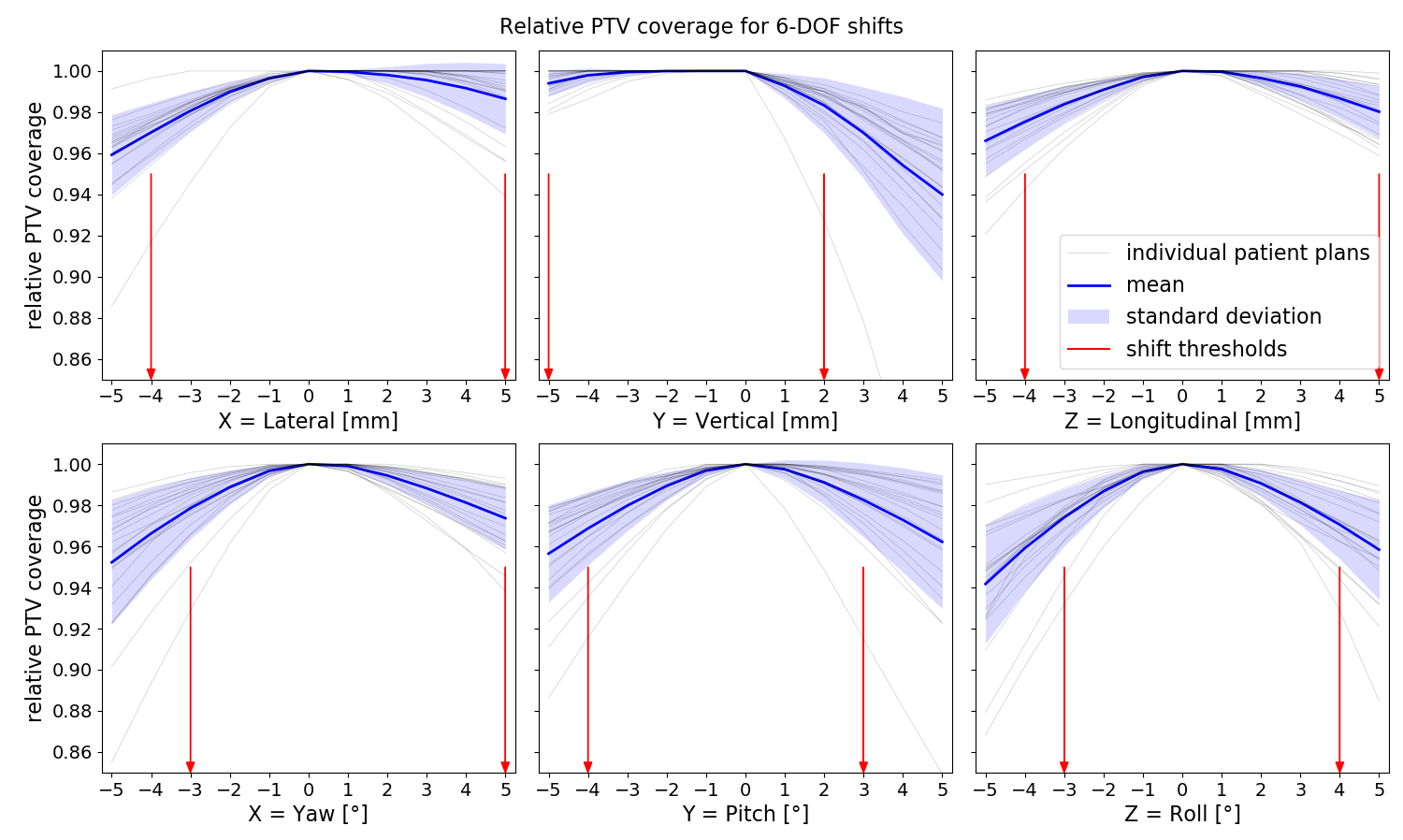
Figure 1 Relative PTV dose coverage for 6-DOF shifts
and shift threshold values
Conclusion
Dosimetric
effects of intrafractional motion during treatment of breast cancer patients
have been evaluated by calculating the dose distribution of the clinical
treatment plans under simulated 6‑DOF shifts. Shift threshold values suitable for
SGRT based monitoring of intrafractional motion were identified. The results underline
the importance of position control during treatment and robust treatment
planning.