parameter vs logfile based 4D proton dose tracking for small movers
Franciska Lebbink,
Germany
PO-1714
Abstract
parameter vs logfile based 4D proton dose tracking for small movers
Authors: Franciska Lebbink1,2, Silvia Stocchiero3, Erik Engwall4, Markus Stock1, Dietmar Georg3, Barbara Knäusl1,3
1MedAustron Ion Therapy Centre, Medical Physics, Wiener Neustadt, Austria; 2Medical University of Vienna, Department of Radiation Oncology, Wien, Austria; 3Medical University of Vienna, Department of Radiation Oncology, Vienna, Austria; 4RaySearch Laboratories AB, Physics, Stockholm, Sweden
Show Affiliations
Hide Affiliations
Purpose or Objective
The motion
compensation strategy in particle therapy depends on the anatomic region,
motion amplitude and underlying beam delivery technology. The prerequisite for
improving existing treatment concepts for moving targets is the quantification of
the interplay effect between organ motion and beam delivery and its impact on
the dose distribution and hence treatment delivery accuracy. While
retrospective logfile based analysis gives insight into the patient’s breathing
and beam delivery time structure, a prospective 4D dose prediction allows adaptation
on a patient specific basis.
Material and Methods
Dose
distributions of 3 pancreas and 3 liver cancer patients with motion amplitudes
below 4mm were analysed. All patients were treated with scanned pulsed proton beams
delivered by a synchrotron. Dose prescription was 5x7.5 Gy(RBE) for pancreas
and 15x4.68 or 10x5 Gy(RBE) for liver. The treatment planning system RayStation8B
(MCv4.2) (RaySearch) was used employing robust optimisation for mitigating
different organ fillings. Treatment accuracy was determined using: (1) file
based 4D dose tracking (f-4DDT) considering the time structure from accelerator
logfiles and surface scanner breathing patterns (C-Rad) for each fraction; (2)
parameter based 4D dose tracking tool (p-4DDT). Input parameters encompassed the
averaged dose rate extracted from the accelerator logfiles over all fractions,
scanning speed as well as constant breathing cycle length. The p-4DDT method was
used additionally to investigate the influence of the starting phase and dose
rate. Both methods considered the given time structures for tracking the static
dose on 8 4DCT phases. This dose distribution was mapped onto the planning CT
using deformable image registration and accumulated for all fractions. DVH
parameters and γ-pass rates with a 2%/2mm criteria were used for dosimetric evaluation.
Results
For the
target structures 4DDT revealed a dose calculation accuracy of 1% for D50%
considering the interplay effect. D98% of the static plan was
disturbed by up to 7% for the PTV and up to 2% for the CTV for 5 out of 6
patients. For liver patients D33%_liver showed deviations between
the two tools up to 14%, while for pancreas patients D1%_stomach varied
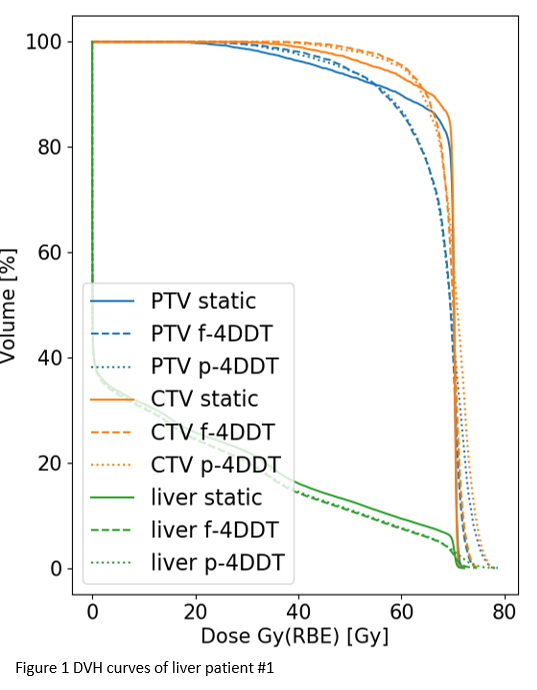
up to 6.5%. The two 4DDT methods agreed within 2% for D98% and D2%
for PTV and CTV for all patients, except for one liver patient where the
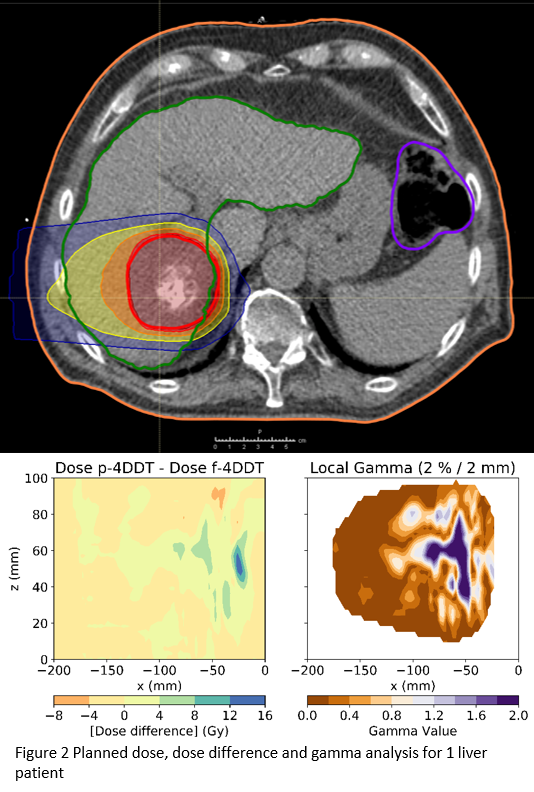
deviation increased up to 7% (Fig1). The γ-pass rates analysis between the p-4DDT and the
f-4DCT showed an agreement above 91% for all patients, confirming the usability
of p-4DDT for dose prediction (Fig2). Variations in starting phase and dose
rate were negligible for the 4DDT outcome.
Conclusion
The p-4DDT
could be used prospectively to determine the impact of beam and organ motion
for pancreatic and liver cases in scanned proton therapy. The systematic
uncertainties covered by the PTV margins compensated well for the motion
effects of the investigated indications preserving an excellent CTV coverage
when motion was considered.