Range shifter air gaps optimized for SGRT on a PBS system for intracranial and thoracic treatments
Laurence Delombaerde,
Belgium
PO-1692
Abstract
Range shifter air gaps optimized for SGRT on a PBS system for intracranial and thoracic treatments
Authors: Laurence Delombaerde1,2, Saskia Petillion2, Robin De Roover1,2, Tom Depuydt1,2
1KU Leuven, Department of Oncology, Leuven, Belgium; 2UZ Leuven, Department of Radiation Oncology, Leuven, Belgium
Show Affiliations
Hide Affiliations
Purpose or Objective
The close proximity
of the movable nozzle and range shifter to the patients’ surface in pencil beam
scanning (PBS) proton therapy of shallow target volumes limits the use of intra
fraction surface guidance systems (SGRT). We have optimized the range shifter
position for five intracranial indications and four thoracic indications to
allow surface guidance and have assessed the impact on plan quality.
Material and Methods
Five patients treated for
intracranial malignancies and two breast and two lymphoma patients were
retrospectively retrieved from our clinical database. PBS intensity modulated proton
therapy (IMPT) plans were generated using a standard minimal range shifter air gap
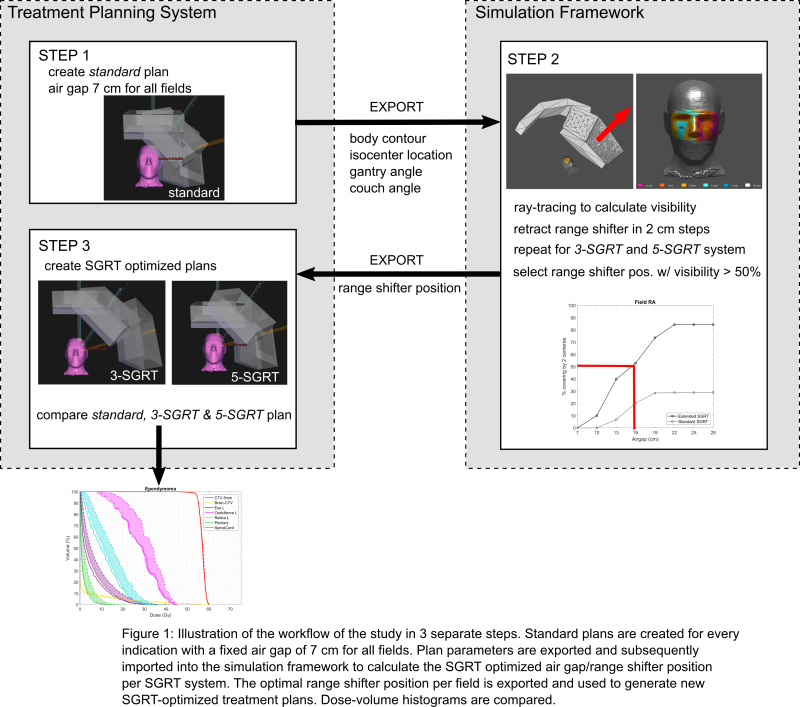
of 7 cm (standard plan). The body
contour and plan parameters (gantry rotation, couch rotation and isocenter)
were imported into a raytracing simulation framework where the visibility of a
region-of-interest (ROI) on the patients surface was calculated for varying range
shifter positions. Two SGRT systems were considered: (a) the commercial three
camera ceiling mounted configuration (3-SGRT)
and (b) a novel conceptual five camera design (5-SGRT). For every treatment field the range shifter position closest
to the patients’ surface was determined were at least 50 % of the ROI was
visible. The optimal parameters were determined for the 3-SGRT and 5-SGRT configuration
and used to create two additional treatment plans, as shown in figure 1. DVHs
were compared between the three plans per indication.
Results
The 3-SGRT system required a
maximally retracted range shifter position for at least one field per plan,
except for one patient. The median air gap was 31 cm (range 7 – 35 cm) for the
3-SGRT and 11 cm (range 7 – 17cm) for the 5-SGRT system. The mean pituitary
dose was 12.2 Gy for the standard, 12.0 Gy for the 3-SGRT and 11.8 Gy for the
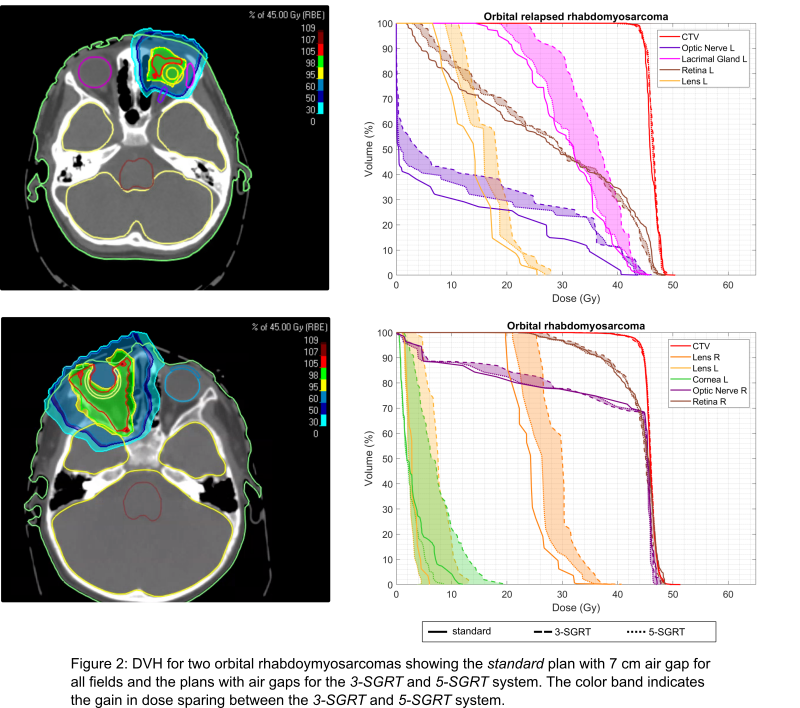
5-SGRT plan. Mean lens dose was 8.9 Gy (L) and 8.2Gy (R) for the standard, 12.0
Gy (L) and 10.8 Gy (R) for the 3-SGRT and 9.3 Gy (L) and 9.0 Gy (R) for the
5-SGRT plan. Mean lacrimal gland dose was 15.5 Gy (L) and 12.9 Gy (R) for the
standard, 16.7 Gy (L) and 13.2 Gy (R) for the 3-SGRT and 15.7 Gy (L) and 13.0
Gy (R) for the 5-SGRT plan. The 5-SGRT plan had a mean dose sparing of 9.9% for
the mean dose to the pituitary gland, 31.0 % and 21.6 % for the mean left and
right lens dose, and 25.2 % and 25.6 % for the mean left and right lacrimal
gland dose, over the 3-SGRT plan. The achievable dose sparing for the 5-SGRT is
shown in figure 2 for two intracranial cases.
Conclusion
Surface guidance
systems can be used during PBS treatment of superficial targets with minimal
loss of plan quality when a dedicated, gantry specific five camera SGRT system is
used. The conventional three camera SGRT system requires the range shifter to
be retracted with a detrimental impact on OAR sparing.