Intra-fraction motion of pelvic lymph node metastases during SBRT
Jorinde Janssen,
The Netherlands
PO-1688
Abstract
Intra-fraction motion of pelvic lymph node metastases during SBRT
Authors: Jorinde Janssen1, Charlotte L. Brouwer1, Floor H. E. Staal1, Stefan Both1, Johannes A. Langendijk1, Shafak Aluwini1
1University Medical Center Groningen, Department of Radiation Oncology, Groningen, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Metastasis-directed radiotherapy (MDRT) using SBRT is highly
recommended for treatment of lymph node (oligo)metastases of prostate cancer.
SBRT is applied using a high fraction dose, steep dose gradients and tight
margins. However, treatment errors are easily induced by patient or target
motion. Patient intra-fraction motion has been reported on previously, however,
intra-fraction motion of lymph node oligometastasis on CBCT has not yet been
described, and current margins are based on individual centre experience. The aim
of this study was to analyse pelvic lymph node motion on CBCT and to derive
margin estimations for SBRT.
Material and Methods
Motion analysis included 18 pelvic lymph node metastases
in 13 patients treated with IGRT in 5 fractions of 7 Gy (every other day) to
the PTV. CBCT linac with 3D couch was used, performing CBCT before and after
each fraction. The entire targeted lymph node (GTV) was delineated by one
observer on planning CT and 179 CBCTs. CBCTs were matched with the planning CT
using a rigid match with verification mask containing adjacent bony anatomy for
translations only. GTV centre of mass displacement was calculated to identify
lesion inter- and intra-fraction translational motions in the left-right (LR),
anterior-posterior (AP) and superior-inferior (SI) patient direction. The
systematic and random population errors were derived, and margins were
calculated (van Herk prescription). Patient bony anatomy intra-fraction motion
was independently included in our calculation. Additionally, we described target
coverage of a 3 mm margin added to the planning GTV using the inclusiveness
index (GTV volume covered / total GTV volume). This inclusiveness index was
derived for all pre- and post-fraction GTV positions.
Results
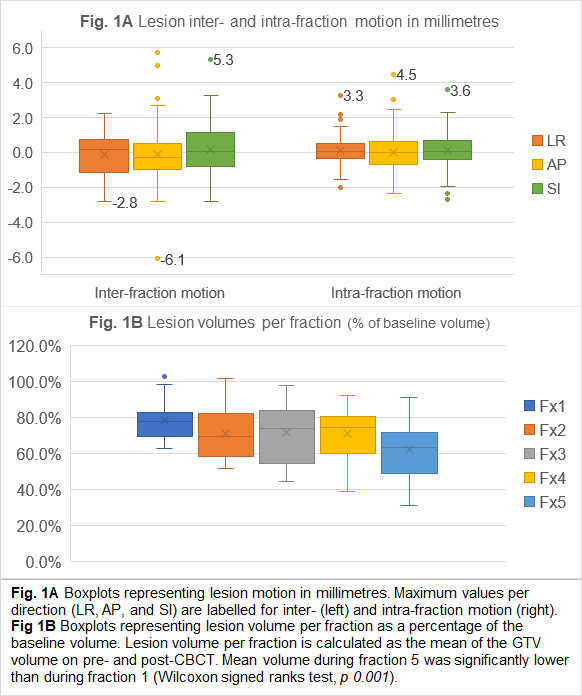
The maximum observed lesion intra-fraction translations
LR, AP and SI were 3.3, 4.5 and 3.6 mm, respectively. (Fig 1A) The mean
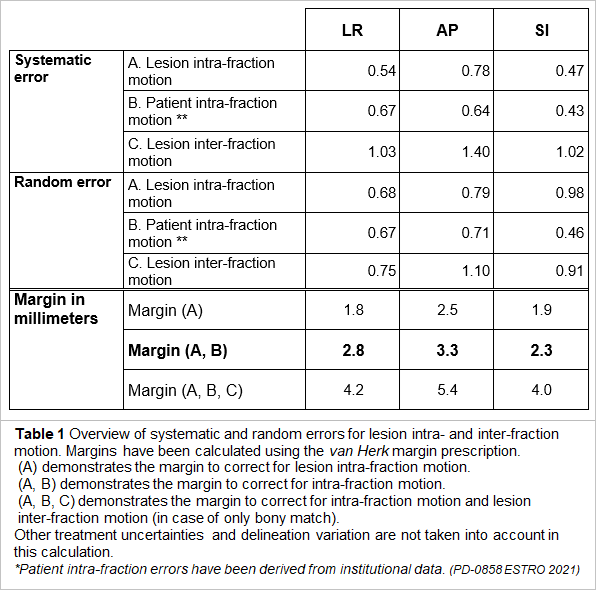
population systematic errors were 0.54 (LR), 0.78 (AP), and 0.47 (SI), and random
errors were 0.68, 0.79, and 0.98. These intra-fraction lesion motion errors
translated in margins of 1.8, 2.5 and 1.9 mm, respectively. Including intra-fraction
patient motion increased the estimated margin to 2.8, 3.3 and 2.3 mm. Lesion
inter-fraction translations were maximum 2.8, 6.1 and 5.3 mm, and including inter-fraction
translations in margin calculation (simulating bony match only) resulted in a
margin of 4.2 (LR), 5.4 (AP) and 4.0 mm (SI). (Table 1)
GTV volume on planning CT ranged from 0.17 cm3 to 3.22 cm3
(median 0.54 cm3). Lesion volume showed a significant decrease
during radiotherapy. (Fig 1B) The expanded GTV (margin 3 mm) had a median
volume of 2.40 cm3, and the mean inclusiveness index was 98.4%. An
inclusiveness index of at least 95% was achieved in 95.9% of all target
positions.