Simultaneous integrated boost in carbon ion radiotherapy: a feasibility study
PO-1655
Abstract
Simultaneous integrated boost in carbon ion radiotherapy: a feasibility study
Authors: Edoardo Mastella1, Silvia Molinelli2, Giuseppe Magro2, Stefania Russo2, Maria Bonora2, Sara Ronchi2, Rossana Ingargiola2, Mario Ciocca2, Barbara Vischioni2, Ester Orlandi2
1CNAO - National Center for Oncological Hadrontherapy, Medical Physics Unit, Pavia, Italy; 2CNAO - National Center for Oncological Hadrontherapy , Clinical Department, Pavia, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
The use of the simultaneous integrated boost (SIB)
in IMRT has been one of the major
technical photon-based RT innovations in the last 20 years, while in carbon ion
radiotherapy (CIRT) a SIB approach has not been fully exploited so far. Until now, at the National Center
for Oncological Hadrontherapy (CNAO, Italy) the standard approach for the treatment of head and neck (HN) adenoid cystic
carcinoma (ACC) has been a sequential (SEQ) strategy consisting of a
first phase of 10 fractions to the low risk (LR)-clinical target volume (CTV)
followed by a second phase of 6 fractions to the high risk (HR)-CTV. In order to improve treatment
planning dose distributions, in this in silico study we investigated the
feasibility of a CIRT-SIB strategy for HN-ACC patients.
Material and Methods
A dataset of 10 ACC patients previously treated with SEQ
irradiation was used. The prescribed dose of the first phase was 41.0 Gy(RBE)/10 fractions to the LR-CTV. A sequential boost phase of 24.6 Gy(RBE)/6 fractions was then delivered in 6
more fractions to the HR-CTV (total prescription of 65.6
Gy(RBE)). In the plan optimization,
the highest priority was sparing the brainstem and optic pathways. The
delivered treatments were re-planned with two SIB dose levels to the LR-CTV:
namely 48.0 Gy(RBE) and 54.4 Gy(RBE). While planning with SIB, the HR-CTV coverage
had higher priority, with fixed organs at risk dose constraints among the SIB
and SEQ plans. The
near-minimum (D98%), the median (D50%) and the near-maximum (D2%) doses were chosen
as dose-summarizing parameters for CTV coverage evaluation together with the homogeneity
(HI) and conformity indexes (CI). The biological effective dose (BED) was
calculated to compare the different fractionation schemes. Statistical significance was assessed with the non-parameter Wilcoxon signed-rank test.
Results
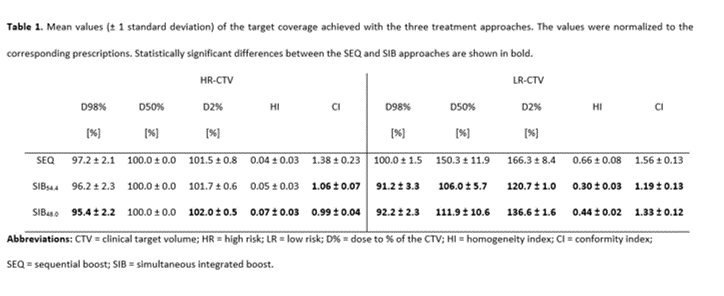
All optimized plans respected the organs at risk dose constraints. For
the HR-CTV, comparable coverage was achieved between the SEQ and SIB54.4,
while with the SIB48.0 the dose inhomogeneity slightly increased
(see Table 1). The HI and
CI values of the LR-CTV decreased significantly for both SIB dose levels,
indicating a better conformality of this technique with respect to the SEQ. With
the SEQ, SIB48.0 and SIB54.4 the LR-CTV median doses were
50.3%, 11.9% and 6.0% higher than the prescriptions.
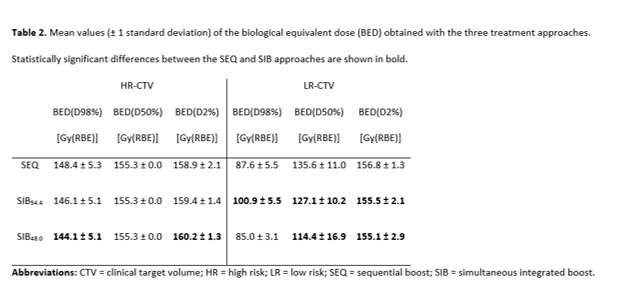
In the LR-CTV, the near-minimum BED(D98%) was comparable between the SEQ
and SIB48.0 (p = 0.19), while a statistically significant increase was found for SIB54.4 plans
(p = 0.002). Significant reduction (p =
0.002) of the median BED(D50%) and near-maximum BED(D2%) was achieved with both
SIB dose levels (see Table 2).
Conclusion
The SIB technique resulted
in highly conformal dose distributions with the reduction of the unintended dose to the LR-CTV. A prescription dose range for the LR-CTV
will be clinically defined to offer tailored personalized treatments, according
to the clinical and imaging characteristic of the patients.