In the observed time frame, 282 patients underwent CT-guided fiducial placement, accounting for 883 implanted fiducials (median 3, range 1-4). Target sites were the prostate bed, extra-spinal bones and pelvic lymph nodes in 158 (56%), 37 (13%) and 87 (31%) patients, respectively. Side effects consisted of minor bleeding at the insertion site and transient pain requiring medication after 24 hours in 5 patients (2%). No grade >2 toxicity was observed, particularly infectious or haemorrhagic complications.
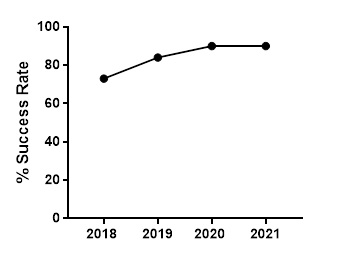
Overall success rate was 86% (719/833); median success rate per procedure was 100% (range 50-100%). Among the 114 fiducials rejected for tracking, failure was due to migration in 63 cases (55%) and misplacement in 51 cases (45%). In the subset of patients receiving ≥3 fiducials (n=161), at least 3 fiducials were used for tracking in 80% (n=129) of patients. Overall success rate increased across the observed time window from 2018 (53/73, 74%) to 2019 (245/293, 84%) to 2020 (246/272, 90%) to 2021 (175/195, 90%) (Figure 2). A consistent, statistically significant improvement in median success rate was observed over time from 2018 (75%, Interquartile Range, IQR 67-100%) to 2019 (100%, IQR 75-100%) to 2020 (100%, IQR 75-100%) to 2021 (100%, IQR 100-100%) : p= 0.0008.