Laparoscopic uterus transposition to preserve fertility in young patients with pelvic radiation
PO-1313
Abstract
Laparoscopic uterus transposition to preserve fertility in young patients with pelvic radiation
Authors: Simone Marnitz1, Michael Püsken2, Andrea Plaikner3, Redouane Fouassi1, Anne Sophie Bereuter1, Christhardt Köhler4
1University Cologne, Department of Radiation Oncology CyberKnife and Radiotherapy, Cologne, Germany; 2University of Cologne, Medical Faculty, Department of Radiology, Cologne, Germany; 3Sklepios-Clinic Hamburg-Altona, Department of Special Operative and Oncologic Gynecology, Hamburg, Germany; 4Asklepios-Clinic Hamburg-Altona, Department of Special Operative and Oncologic Gynecology, Hamburg, Germany
Show Affiliations
Hide Affiliations
Purpose or Objective
Anal/rectal cancer in women younger than 40 years is a rare event. However, due to high radiosensitivity of ovaries and endometrium pelvic radiation is inconsistent with fertility preservation.
Material and Methods
Anastomosis between uterine and ovarian arteries provide sufficient blood supply to the uterus even after transsection of both uterine arteries. Thus, uterus can be released from all vaginal and parametrial attachments without impairment of uterine perfusion. After meticulous laparoscopic pelvic dissection and preservation of infundibulopevic ligaments mobile uterus together with both adnexae will be fixed on the anterior abdominal wall above the umbilicus with non-resorbable sutures (Figure 1). Finally, cervix uteri will be sutures to a 3cm umbilical fascia window to ensure menstruation and cervical secretion.
Results
Two patients
were treated with uterus transposition (n=1) with total transposition as described,
n=1 with anterior transposition). There was no severe perioperative morbidity. Patients
underwent a neoadjuvant short course radiation (5x5Gy; n=1) and a primary chemo-radiation
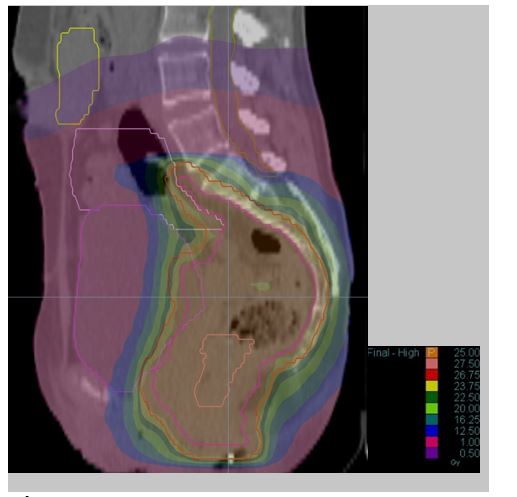
(1.8-59.4Gy; n=1). The dose distribution for the patient with the upper transposition
showed the uterus and the ovaries within the 0.5 Gy isodose (Figure 2). Two years
after anterior transposition, after an uneventful
course of pregnancy after in vitro fertilization, primary cesarean section was
performed at 37 weeks + 6 days of gestation1.
Conclusion
Anterior or upper uterus transposition offers the possibility to young women with pelvic malignancies to preserve ovarian function as well as to keep the endometrial dose within the uterus very low. This allows a pregnancy and successful delivery after cancer treatment.
Figure 1: Sagittal MRI of the patient after total uterus
transposition. The cervix is located in the umbilicus.

Figure 2: Dose distribution of radiation planning for
short term neoadjuvant radiation for the patient with the uT3 N+ rectal cancer.
Yellow= uterus. 0.5 gray isodosis covers the half of the uterus (purple volume),
one gray isodose can be kept below the uterus (margenta).
References
1. Köhler C, Marnitz S, Biel P, Cordes T. Successful Delivery in a 39-Year-Old Patient with Anal Cancer after Fertility-Preserving Surgery Followed by Primary Chemoradiation and Low Anti-Mullerian Hormone Level. Oncology 2016;91:295-8.