Acute toxicity of hypofractionated locoregional radiotherapy in advanced breast cancer
PO-1177
Abstract
Acute toxicity of hypofractionated locoregional radiotherapy in advanced breast cancer
Authors: Roberta Tummineri1, Andrei Fodor1, Flavia Zerbetto1, Marcella Pasetti1, Chiara Lucrezia Deantoni1, Ariadna Sanchez Galvan2, Roberta Castriconi3, Paola Mangili3, Antonella Del Vecchio3, Nadia Gisella Di Muzio4
1IRCCS San Raffaele Scientific Institute, Radiation Oncology, Milano, Italy; 2Milano-Bicocca University, Radiation Oncology, Milano, Italy; 3IRCCS San Raffaele Scientific Institute, Medical Physics, Milano, Italy; 4IRCCS San Raffaele Scientific Institute - Università Vita-Salute, Radiation Oncology, Milano, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Hypofractionated whole
breast radiotherapy is considered the standard after conservative surgery for
breast cancer (BCa), but the interest in hypofractionation is growing even for locoregional
treatments, involving not only breast/chest wall, but also lymph nodal (LN)
areas. We report acute toxicity in patients with advanced BCa treated with hypofractionated
radiotherapy (HRT) to breast/chest wall and regional LN in our Institute.
Material and Methods
From
03/2018 to 05/2021 132 pts with diagnosis of advanced BCa pts (98% female, 2%
male) underwent locoregional HRT after conservative surgery (58%) or mastectomy
(40.5%), and 3 pts received radical
RT (1.5%). Two pts had
bilateral BCa (134 irradiated breasts). Median age was 52 (26-86) years. Molecular
subtypes were: Luminal A 29%,
Luminal B Her2- 28.5%,
Luminal B Her+ 19%, HR negative Her2+ 13% and Triple negative 10.5%. Neoadjuvant chemotherapy was prescribed in 55% of pts, adjuvant in 55%, and concomitant in 11%. Adjuvant
hormonal therapy was prescribed in 76% of pts (IA or TMX -/+ LH-RH analogue).
Thirty-three % of pts underwent HER2-targeted therapy. Treatments were delivered with 3DCRT (11%), VMAT
(30%) or Tomotherapy (59%, TomoDirect or TomoHelical), to a total dose of 40.05
Gy in 15 fractions, delivered in 3 weeks, to breast/chest wall and regional
LNs. A simultaneous integrated boost (SIB) up to 48 Gy to the tumor bed was
delivered for pts with high-risk local relapse. The target was: whole breast in
60% (46% right, 54% left), chest wall in 40% (40% right, 60% left, 33% without and
67% with post-mastectomy reconstruction), supraclavicular LN in 100%, axillary LN in 34.4%, and internal
mammary chain in 13.5% of cases, respectively. A SIB to the tumor bed was
delivered in 34.5% of pts. Acute
toxicity was registered according to CTCAE v 4.0.
Results
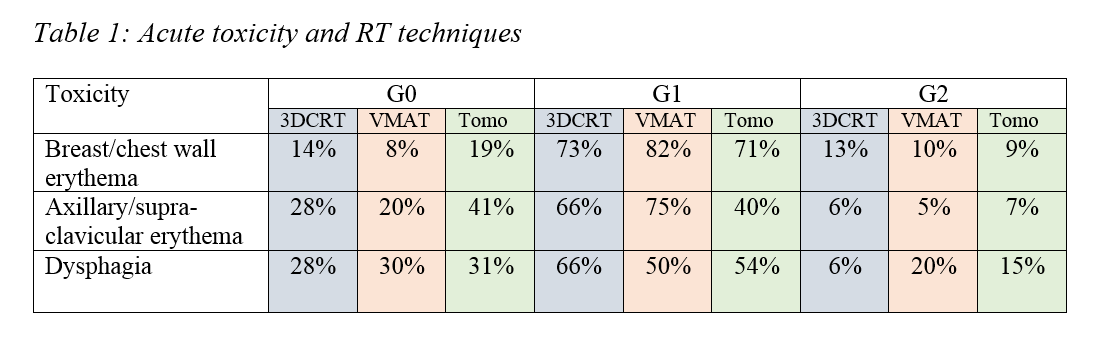
Acute
toxicity is summarized in table 1. No patient experienced ≥G3 acute toxicity. No
significant differences in toxicity were found between the different RT
techniques. G2 skin toxicity was experienced in
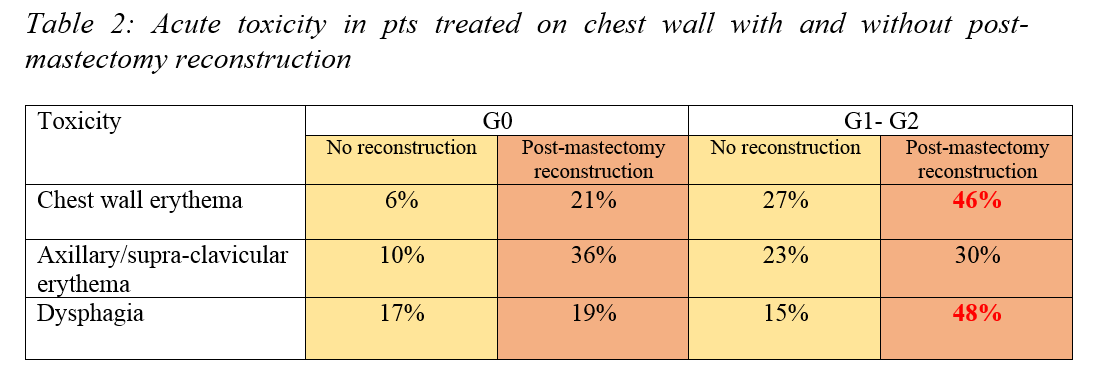
13% of pts with SIB and 8% without SIB. Significant increase of G1-G2 skin
toxicity and dysphagia were found in pts treated on chest wall with
post-mastectomy reconstruction (as summarized in table 2).
Conclusion
Locoregional
HRT is feasible with low acute toxicity without significant differences in toxicity between the
different RT techniques.
Longer follow-up is needed to evaluate late toxicity and local control in the different subgroups of patients.