Fiducial motion relative to tumor bed in partial breast irradiation and risk of geographical miss
PD-0779
Abstract
Fiducial motion relative to tumor bed in partial breast irradiation and risk of geographical miss
Authors: Nienke Hoekstra1, Steven Habraken1, Annemarie Swaak - Kragten1, Jean-Phillipe Pignol2, Mischa Hoogeman1
1Erasmus MC Cancer Institute, Radiotherapy, Rotterdam, The Netherlands; 2Dalhousie University, Radiotherapy, Halifax, Canada
Show Affiliations
Hide Affiliations
Purpose or Objective
The trend
towards partial breast irradiation (PBI) and increased hypofractionation stresses
the importance of the geographic accuracy of radiation delivery. As there are
fewer fractions to compensate for a geographical miss in one fraction, the risk
of local recurrence might increase. Furthermore, the increased use of full
thickness closure leads to a seroma that is often not clearly visible on daily
imaging. Fiducials are used as surrogates for patient positioning. To assess
the accuracy of treatment delivery in this situation, we investigated the
motion of fiducials relative to the tumor bed, assuming patients would be treated
with single fraction PBI. Possible geographical miss and compensation for this
error are evaluated by calculating CTV to PTV margins.
Material and Methods
Sixty-eight patients
treated in a Cyberknife PBI cohort study were included. All patients had a
minimum of 3 titanium surgical clips placed in the tumor bed during lumpectomy. They
also had 3 interstitial gold markers inserted postoperatively around the tumor
bed under US guidance. A planning CT and a diagnostic-quality in-room CT at the
first fraction were made with identical scanning parameters with a median
interval of 15 days. The two CT scans were co-registered on the tumor bed area using
MIM 6.9.3 software. The residual displacement was calculated for each fiducial individually
and for the center of mass (CoM) of all interstitial markers and all surgical
clips. These errors were used to calculate the uniform three-dimensional CTV to
PTV margin required for the motion of the fiducials relative to the tumor bed.
We calculated margins varying the percentage of patients with a completely
covered CTV during treatment. We used the 2-sample Kolmogorov Smirnov test to
compare the error distributions for the two fiducial types.
Results
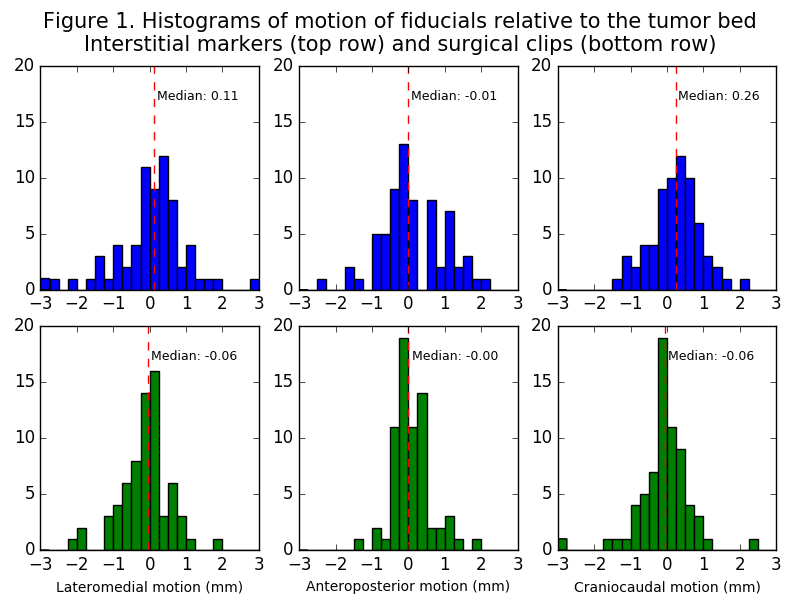
The
distributions of the motion of the CoM per fiducial type relative to the tumor
bed are shown in figure 1. The distributions were significantly different for
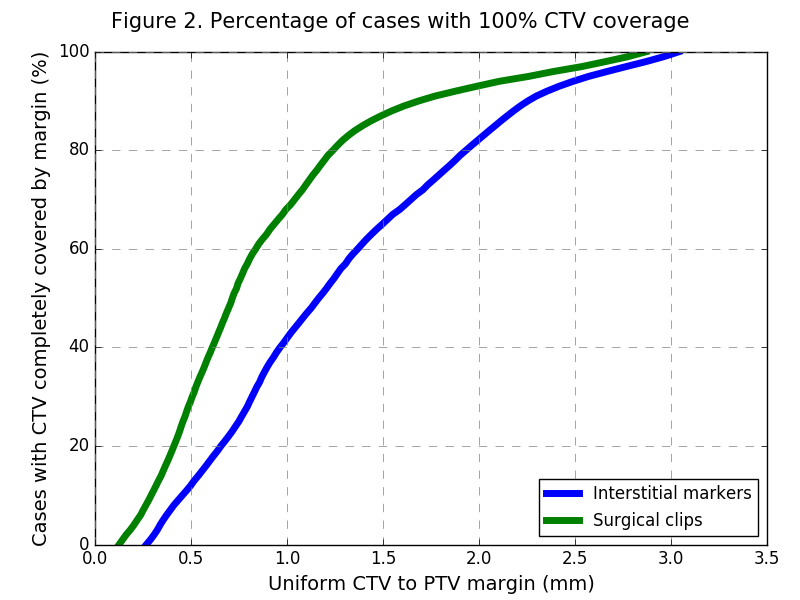
the two fiducial types (p < 0.001). In figure 2, the margin is plotted
against the percentage of patients with 100% CTV coverage. The uniform margin
required to compensate for fiducial motion in 90% of patients was 2.3 mm for
the interstitial markers and only 1.7 mm for the surgical clips. Applying this margin
of 2.3 mm to positioning based on surgical clips would result in 95% of
patients with 100% CTV coverage.
Conclusion
There is substantial
fiducial CoM motion relative to the tumor bed between simulation and PBI treatment.
Its magnitude was influenced by the type of fiducial. The margin required to
cover the CTV of 90% of patients was 2.3 mm for positioning based on
interstitial markers. This margin would cover the CTV of 95% of patients if
surgical clips were used, potentially decreasing the risk of local recurrences.
Our method of calculating the percentage of patients with 100% coverage for
each margin allows for an informed decision on the trade-off between irradiated
volume and risk of geographical miss.