Feasibility CBCT-based online adaptive 5x5Gy radiotherapy for neoadjuvant rectal cancer treatment.
Marije Frank,
The Netherlands
OC-0618
Abstract
Feasibility CBCT-based online adaptive 5x5Gy radiotherapy for neoadjuvant rectal cancer treatment.
Authors: Marije Frank1, Rianne de Jong1, Jorrit Visser1, Niek van Wieringen1, Jan Wiersma1, Debby Geijsen1, Arjan Bel1
1Amsterdam UMC location AMC, Radiation Oncology, Amsterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Online adaptive radiotherapy has
the potential to reduce toxicity for patients because it enables margin
reduction around the clinical target volume (CTV). This study describes and
evaluates for the first time a Conebeam CT (CBCT)-based online adaptive workflow
for rectal cancer in the neo adjuvant setting with respect to timing of
different steps in the process, plan quality, target coverage and patient
compliance.
Material and Methods
Fifteen consecutive 5 x 5Gy
rectal cancer patients were treated on a ring-based linear accelerator (Ethos,
Varian, Palo Alto, USA). Relatively small margins of 5 mm were applied to the
CTV (consisting of mesorectum, pre sacral space and elective lymph nodes) in AP
and LR direction. For the cranial and caudal borders a margin of 8 mm in CC
direction was applied (Figure 1). The Ethos operates as an integrated platform
for both treatment planning and delivery. A reference plan was generated based
on a single planning CT. After setting up the patient the adaptive procedure
started with the acquisition of a CBCT. The reference CT scan was registered to
the CBCT using deformable registration creating a synthetic CT scan. With the
support of artificial intelligence and structure guided deformation contours
were adapted by the system to match the anatomy on the CBCT (Figure 1). If
necessary, these contours were adjusted. Subsequently a new plan was generated
on the synthetic CT scan. A second and third CBCT were acquired to check target
coverage of this new plan just before and after treatment delivery,
respectively. Treatment was delivered using volumetric modulated arc treatment
(VMAT). For this introduction phase, a team consisting of 2 RTTs, a physician
and a physicist was present at the linear accelerator for each procedure. RTTs
were in charge of running the system. All steps in this process were timed.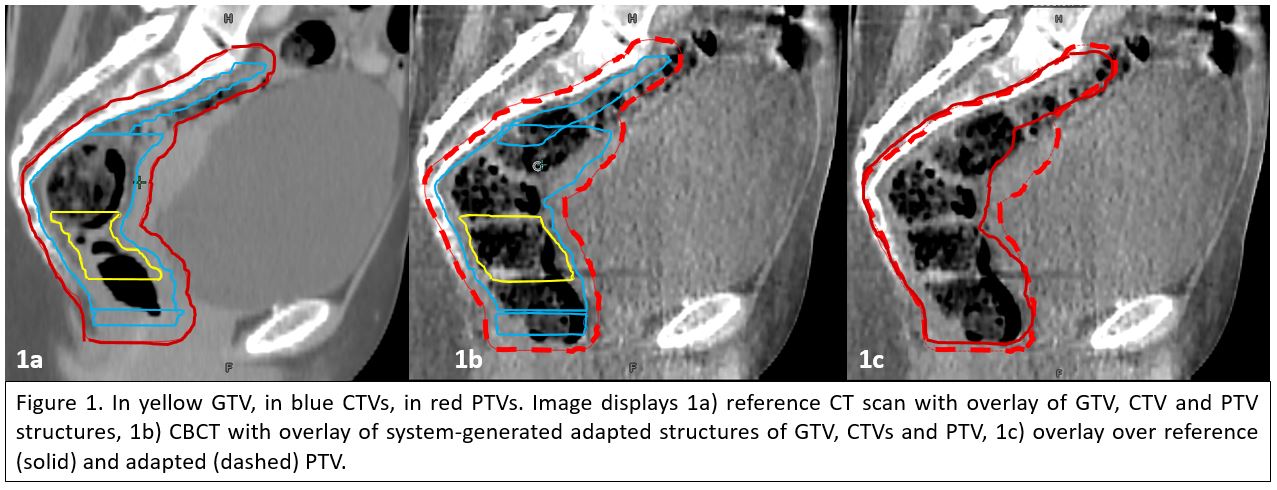
Results
On average the time slot needed
at the treatment machine was 34 minutes. The process of acquiring a CBCT,
evaluating and adjusting the contours, creating the new plan and verifying the
CTV on the CBCT scan took on average 20 minutes. Including delivery and post
treatment verification this was 26 minutes. The system-generated target volumes
needed user adjustments in 50% of fractions. Target volumes on second
pretreatment CBCT were all covered with the 95% isodose line. The number of
monitor units (MU) of the adapted plan never deviated more than 15% from the
number of MU of the reference plan. Patient compliance with respect to bladder
filling and total treatment time was excellent.
Conclusion
First clinical experience with CBCT-based
online adaptive radiotherapy shows it is feasible and suitable for hypo fractionated
rectal cancer treatment.