First VMAT delivery with MLC-tracking for single and multi fraction lung SBRT on a Unity MR-linac
Prescilla Uijtewaal,
The Netherlands
OC-0616
Abstract
First VMAT delivery with MLC-tracking for single and multi fraction lung SBRT on a Unity MR-linac
Authors: Prescilla Uijtewaal1, Pim Borman1, Peter Woodhead1,2, Charis Kontaxis1, Sara Hackett1, Joost Verhoeff1, Bas Raaymakers1, Martin Fast1
1UMC Utrecht, Radiotherapy, Utrecht, The Netherlands; 2Elekta AB, Elekta AB, Stockholm, Sweden
Show Affiliations
Hide Affiliations
Purpose or Objective
Conventional lung SBRT requires large treatment
margins to cover tumor motion resulting from respiration. This may avoid
underdosage but increases toxicity risks. To maximize healthy tissue sparing,
we previously developed MRI-guided MLC tumor tracking for the 1.5 T Unity
MR-linac (Elekta AB, Stockholm, SE) in combination with IMRT. Recently, we also
piloted VMAT deliveries on Unity to further maximize plan conformality and
delivery efficiency. In this study, we demonstrate the feasibility of a first
experimental setup on an MR-linac that combines VMAT with MLC-tracking for a
range of lung SBRT indications.
Material and Methods
All experiments were performed on a 1.5 T Unity
MR-linac in research mode.
A Quasar MRI4D phantom (ModusQA, London, CA) was used
to generate: no motion (static reference), Lujan motion (cos4,
peak-to-peak amplitude A = 20 mm, f = 0.25 Hz), and subject-derived real
respiratory motion (average A = 11 mm, average f = 0.33 Hz) with an average
baseline drift of 0.6 mm/min. The phantom contained a film insert with a 3 cm
spherical target (GTV) that could be positioned centrally or 10 cm off-center
(peripheral) in a water-filled body oval. Target positions were continuously
estimated from 2D cine-MR (4 Hz). A linear regression prediction filter compensated
for system latency. Predicted positions were used continuously to realign the MLC
with the target position.
We created three VMAT treatment plans with 3 mm
GTV-to-PTV margins following the clinical planning template for lung SBRT: a
central plan (8x7.5 Gy) and two peripheral plans (3x18 Gy and 1x34 Gy).
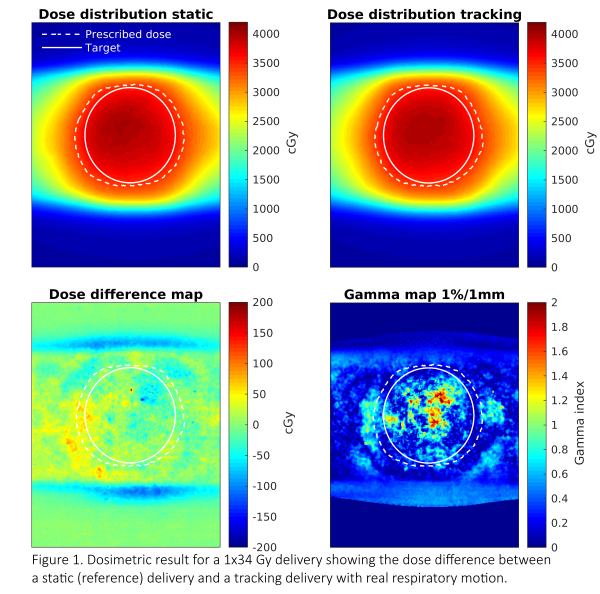
Gafchromic EBT3 or EBTXD films were used to measure the delivered dose. A
1%/1mm local Gamma-analysis quantified dose differences between the static
reference and tracking cases. Additionally, the dose area histogram (DAH) was
determined for the target.
Results
The VMAT plans had a conformity index (prescribed isodose
volume/ PTV) of 1.4-1.5 and an MU-weighted mean-field area of 13-16 cm2.
Treatment delivery times were: 6.7 min, 13.1 min, and 24.2 min, for the 8x7.5
Gy, 3x18 Gy, 1x34 Gy lung SBRT plans respectively. The plans required an RMS leaf
speed of 0.5-0.7 cm/s. Tracking required a maximal additional 2.4 cm/s leaf
speed. Each plan was delivered in respectively 2, 4, and 6 arcs.
The local gamma analysis for the central delivery
shows that MLC-tracking improved the gamma pass-rate from 67.5% to 98.3% for
Lujan motion and to 94.2% for the real respiratory trace. For peripheral
deliveries with real respiratory motion, the 3x18 Gy delivery had a 97.3%
pass-rate and the 1x34 Gy delivery had a 96.8% pass-rate (Fig.1).
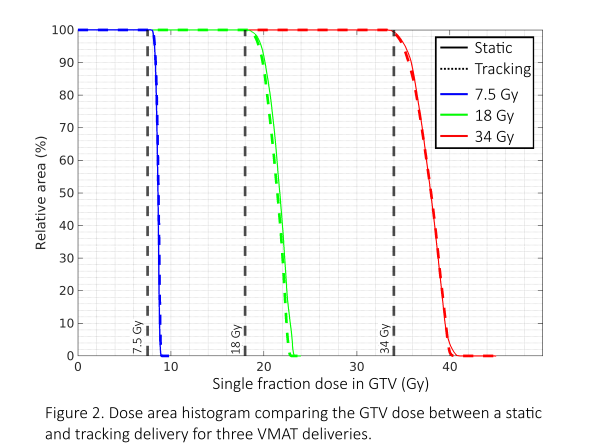
The DAH (Fig.2) shows that the target dose agrees well
between static and tracking deliveries with real respiratory motion. The figure
also shows that the minimum dose in the target is well above the prescribed
dose.
Conclusion
We provided a first experimental demonstration
of the technical feasibility of VMAT combined with MR-guided MLC-tracking for
central and peripheral lung SBRT.