Nine years of plan libraries for locally-advanced cervical cancer patients: what have we learned?
Dominique Reijtenbagh,
The Netherlands
OC-0613
Abstract
Nine years of plan libraries for locally-advanced cervical cancer patients: what have we learned?
Authors: Dominique Reijtenbagh1, Jérémy Godart1, Joan Penninkhof1, Sandra Quint1, András Zolnay1, Jan Willem Mens1, Mischa Hoogeman1
1Erasmus MC, Radiation Oncology, Rotterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Our center
has been using a library-based plan of the day (PotD) strategy for EBRT for
locally advanced cervical cancer patients since 2011. The goal of this strategy
is to reduce dose to normal tissue. Since 2011, various adjustments have been
made to the PotD and the treatment protocol. However, the performance of the
PotD has not been assessed longitudinally. This study analyzes PotD performance
over nine years and compares it to a maximum attainable normal tissue sparing
based on daily replanning.
Material and Methods
All patients
clinically treated with the PotD protocol were included. As part of the
protocol, patients were categorized as movers or non-movers based on
tip-of-uterus displacement between an empty and full bladder CT scan. Non-movers
and movers received one and two personalized library plans respectively, based
on a motion model constructed from the full and empty bladder CT scan. An additional
motion-robust plan (PTVBU) was available for all patients. Starting
date of radiotherapy, selected plans, and frequency and reason for full
replanning were registered. Full replanning (new planning CT scans and plan
library) was performed when PTVBU was selected three or more times during treatment.
Planning
structures were collected. Weighted PTV volumes (PTVw) were calculated
for all patients using the weighted sum of the PTV volumes from the library plans
actually used for the fractions. This was considered representative for
clinical practice. A fully-online adaptive strategy was simulated for each
patient (PTVfully adapt.), which comprised the full-bladder CTV and elective
CTV with a 5-mm margin.
The performance
of the protocol was assessed by the percentage of patients requiring full replanning,
the percentage of used motion-robust plans, and the comparison between the PTVw,
PTVBU and PTV fully-adapt. volumes.
Results
A total of
376 patients was treated between January 2011 and May 2020, of which 18%
required full replanning. 52% of these cases was attributable to shortcomings
of the motion model. The total use of back-up plans decreased from 20% from
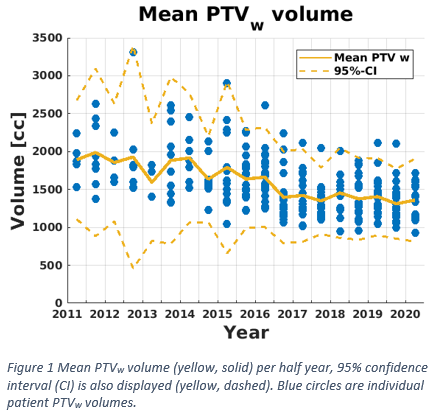
2011 to 5-10% beyond 2014. Figure 1 shows that this and protocol adjustments
have improved the PotD strategy over time, resulting in a mean decrease of 500
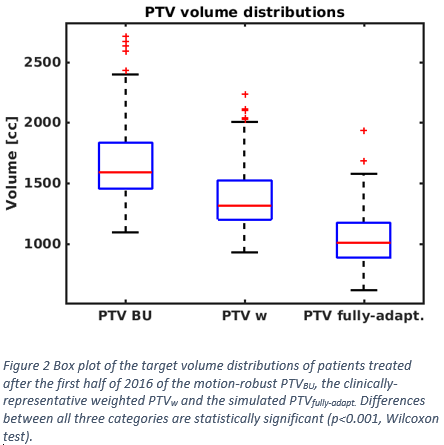
cc in PTVw volume. A stabilization is visible after 2015. Figure 2 displays
the boxplots of the PTVBU, PTVw, and PTVfully adapt of
patients treated in the second half of 2016 and later. This figure illustrates that the use of the
plan library decreased PTVw with 17% compared to PTVBU
and that a fully online-adaptive strategy could increase this reduction to 37%.
Conclusion
This
long-term analysis shows that plan-library-based PotD can consistently reduce
PTV volume by 17%. Further reduction is possible, but at the expense of a
higher workload.