Applying column generation to the intensity-modulated high-dose-rate brachytherapy inverse planning
OC-0042
Abstract
Applying column generation to the intensity-modulated high-dose-rate brachytherapy inverse planning
Authors: Majd Antaki1, Marc-André Renaud2, Jan Seuntjens1, Shirin A. Enger1
1McGill University, Department of Oncology, Montreal, Canada; 2Polytechnique Montréal, Department of Mathematical & Industrial Engineering, Montreal, Canada
Show Affiliations
Hide Affiliations
Purpose or Objective
Intensity
modulated high dose rate brachytherapy (IMBT) is a rapidly developing
application of brachytherapy where anisotropic dose distributions can be
produced at each source dwell position. This technique is made possible by
placing rotating metallic shields inside brachytherapy needles or catheters. By
dynamically directing the radiation towards the tumours and away from the
healthy tissues a more conformal dose distribution is created at the expense of
increasing complexity of the treatment planning process. In this study column
generation method is investigated for IMBT treatment plan optimization.
Material and Methods
A
column generation optimization algorithm is developed to optimize the dwell
times and shield angles. At every iteration, the plan is optimized with the
chosen dwell position and shield angle (DPSA) combinations and the DPSA that
would best improve the cost function at every iteration is added to the plan.
The optimization process can be stopped when the clinical plan evaluation
criteria have been met to limit the plan complexity. In this work the
optimization was stopped when no more DPSAs is expected to add value to the
current plan.
Results
The
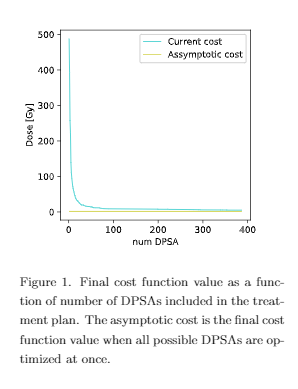
column generation approach yielded a near-optimal treatment plan with 387 DPSAs
from 2080 possible DPSAs for a prostate case. The final iteration contained a
plan with a complexity five times smaller than the original one. Figure 1 shows
that the cost function converges to the asymptotic cost, which is the cost when
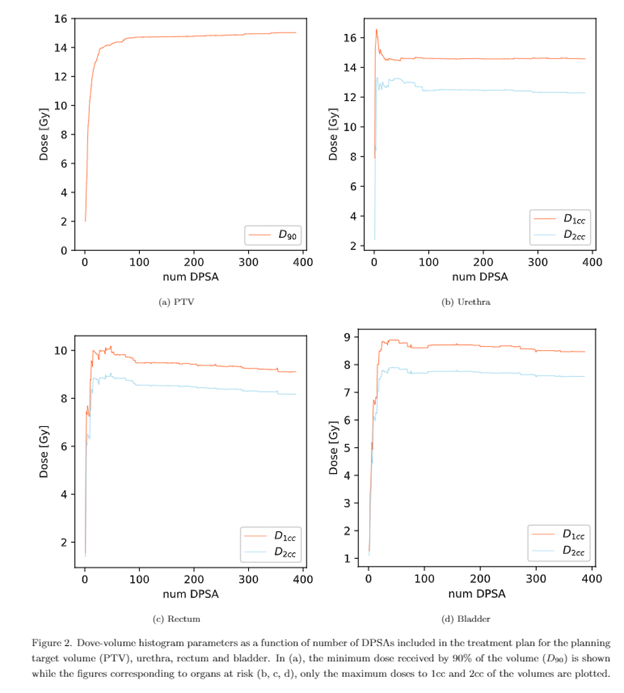
all DPSAs are included in the optimization. Figure 2 illustrates the dosimetric
indices of interest at each iteration. After some fluctuations D1cc and D2cc of
the organs at risk (OAR) reach their maxima during the first 50 iterations,
then decrease to stabilize after 100 iterations. With the D2cc of both the
bladder and the rectum being below 10 Gy, and the D1cc of the urethra below 15
Gy, the dosimetric requirement for the OAR are satisfied while still having
V100 > 15 Gy in the planning target volume.
Conclusion
The
column generation method produced a high-quality deliverable prostate IMBT
plan. The treatment plan quality eventually reached a plateau where adding more
DPSAs had a minimal effect on dose volume histogram parameters. The iterative
nature of the column generation method allows early termination of the
treatment plan creation process as soon as dose volume histogram parameters
satisfy their clinical requirements or if they have stabilized.