COMPARISION OF TWO HDR INTRACAVITARY BRACHYTHERAPY REGIMENS IN TREATMENT OF CERVICAL CANCER
OC-0062
Abstract
COMPARISION OF TWO HDR INTRACAVITARY BRACHYTHERAPY REGIMENS IN TREATMENT OF CERVICAL CANCER
Authors: Abhishek Krishna1, Hasib AG1, Donald Fernandes1, Athiyamaan MS2, Sandesh Rao1, Sharaschandra Shankar1
1Father Muller Medical College, Radiation Oncology, Mangalore, India; 2Father Muller Medical College, radiation Oncology, Mangalore, India
Show Affiliations
Hide Affiliations
Purpose or Objective
Carcinoma
of the uterine cervix is one of the common malignancies among Indian women. Radiation therapy including external beam radiotherapy(EBRT) and intracavitary brachytherapy (ICBT) plays a pivotal role in patients with locally advanced disease. HDR
ICBT for carcinoma of the cervix is now well established because of its various
advantages. Although there are three decades of published literature on the
efficacy of HDR brachytherapy, optimum time, dose, and fractionation is not
very well defined. Two fractions of high-dose-rate brachytherapy are convenient for
patients, but most radiation oncologists fear that they could lead to excessive
rectal or bladder toxicity.
The objective of this study was to assess and compare the local
control and toxicities between HDR Intracavitary
Brachytherapy with 7.5 Gy per fraction in three fractions (Arm A) and 9 Gy per fraction in two fractions (Arm B) post
EBRT in treatment of carcinoma cervix.
Material and Methods
A total of
180 patients meeting the inclusion criteria were included in the study and
randomly assigned to 2 arms of 90 patients each. All patients received concurrent chemoradiation to a dose of 50 Gy in 25 fractions along with weekly cisplatin. Post chemoradiation, arm A received HDR ICBT with a dose of 7.5 Gy per fraction, 1 fraction per week for 3 fractions and arm B received HDR ICBT 9 Gy per fraction , 1 fraction per week for 2
fractions. Patients were evaluated monthly for assessment of local control and toxicities.
Statistical evaluation was done with mean, percentage and frequency using Chi Square ,
Student T test.
Results
180 patients were included in the study with 90 patients in each arm. The total duration of
treatment was
significant less in Arm B compared to Arm A (59 days vs 68 days, p<0.0001). 80
(89%) patients in arm A, had complete response at 6 months. 2(2.2%) patients had partial response and 4(4.4%)
patients had local recurrence. In Arm B, 87 (96.7%) of the patients had
complete response and was statistically significant (p=0.040).
2(2.2%) patient had local recurrence in the cervix.
Grade 2 and above diarrhea was seen in 4.4% of the patients in arm A and in 7.7% of patients in arm B. Grade
2 and above proctitis was seen in 3.3 % of the patient in arm A and in 6.6 % of the
patients in arm B. One patient in arm B had Grade 4 proctitis. Grade 2 urinary tract pain was seen in 10 (11.1%) patients in arm A and in 6 (6.7%) patients in arm B. One patient each in arm A and arm B had grade 1
hematuria. 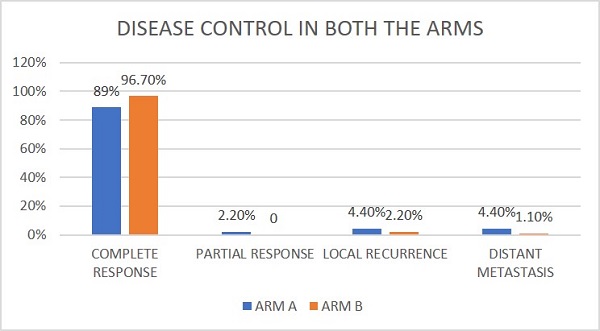
Conclusion
This study, with intracavitary brachytherapy with 9 Gy in 2 fractions showed a better local control of tumour compared to 7.5 Gy in 3 fractions. Although there was no statistical significance, our study showed a slightly higher rate of rectal toxicities in the 9 Gy arm which could be managed medically. The study also highlighted the need for completion of total treatment of EBRT and brachytherapy within 60 days to reduce the recurrence rates.