commissioning of a Venezia applicator: discrepancies between expected and actual source positions
PO-0202
Abstract
commissioning of a Venezia applicator: discrepancies between expected and actual source positions
Authors: Naiara Fuentemilla1, Aitor Fernandez1, Santiago Pellejero2, Rocío Estrada2, Jesus Escobar2, Laura Bragado2, Fernando Caudepon2, Fernando Mañeru2, Santiago Miquelez2, Elena Villafranca3, Marta Barrado3
1Complejo Hospitalario de Navarra, Servicio de Radiofísica Hospitalaria y PR, Pamplona, Spain; 2Complejo Hospitalario de Navarra, Servicio de Radiofísica y PR, Pamplona, Spain; 3Complejo Hospitalario de Navarra, Servicio de Oncologia Radioterapica, Pamplona, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
The Venezia Advanced Gyneacological applicator
developed by Elekta is an insterstitial-intracavitary hybrid applicator. This
work reports on some discrepancies encountered between the expected dwell
positions and the actual source positions in the commissioning process of the
26 mm diameter Venezia applicator.
Material and Methods
We obtained and compared the most distal source
position in relation to the applicator by three methods: i) using the Oncentra applicator
library (central path (C) and “real” source path (SP)); ii) by auto-radiography
(AR) using Gafchromic EBT3 (a distance of 1300 mm was entered following
manufacturer specifications); and iii) X-Ray imaging (RX) with the Varian OBI
imaging system. For the last, the source trajectory was reproduced with a dummy
source and the applicator was held in horizontal position in order to simulate
clinical conditions.
Results
A relevant deviation from the expected was
detected for the first position in the semilunar ovoid 2 (Ov2, table 1) when
using auto-radiography: 3mm to that predicted by SP. After further
investigation, we determined that the source was not able to reach positions
beyond the 4th position, which resulted in an overdosage at that
position. This problem was attributed to internal friction, although Flexitron
did not warn about any obstruction.
| Geometry | Ov1 (mm) | Ov2(mm) |
| Central | 6.4 | 6.4 |
| Source path | 6.8 | 6.8 |
| X-ray | 5.6 | 6.6 |
| Autoradigraphy | 6.6 ± 0.1 | 9.8 ± 0.1 |
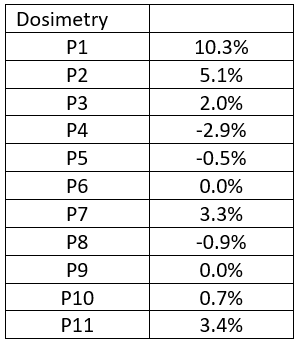
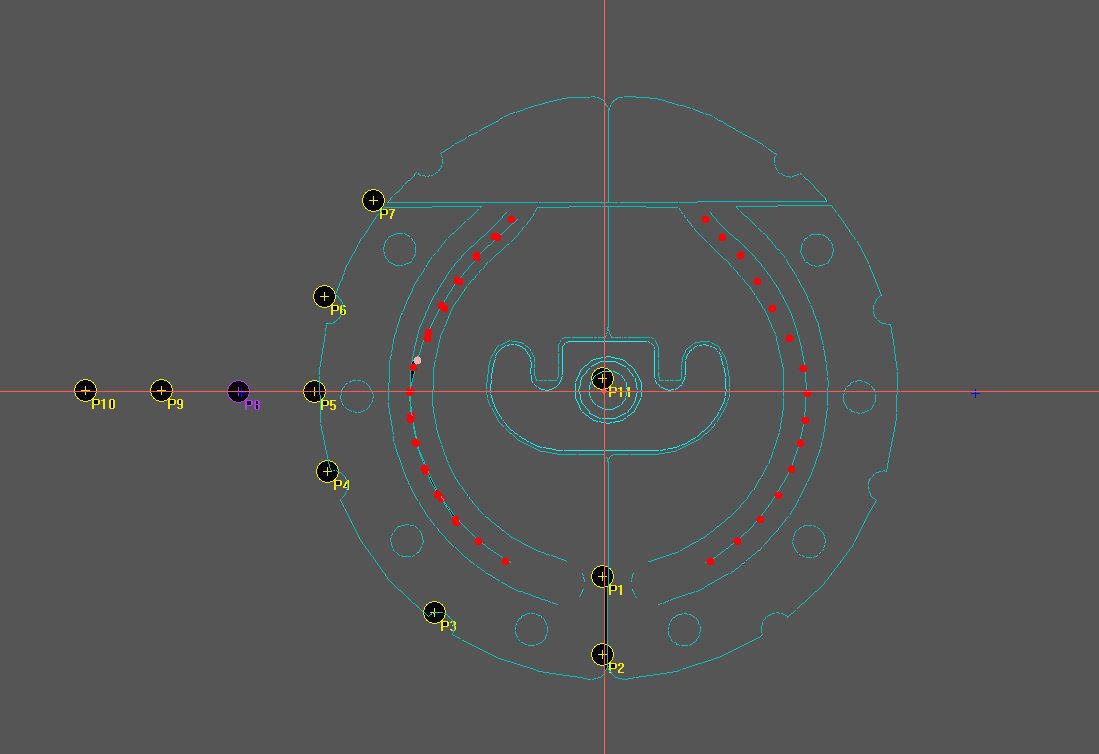
In
order to establish possible clinical implications if the defect had not been
detected, we calculated differences in dose delivery (shown in table 2) at
several points around the applicator (image 1). Calculation was performed using
the TG43 algorithm implemented in OncentraBrachy 4.5.3. treatment planning
system.
Conclusion
Despite the resulting dosimetric differences not
being relevant clinically in principle (points 3 to 10), the Ov2 was replaced with
a new one. The commissioning of the new Ov2 resulted in no important geometric discrepancies
(less than 1mm).
Brachytherapy
entails a lot of uncertainties, so all personnel involved should ensure that
uncertainties are minimized. Specifically, the medical physicist should perform
the necessary measures to know in detail their applicators and ensure that they
are suitable for clinical use.