Margins based on inter-fractional surgical clip movement for breast tumor bed radiotherapy boost
Karina Lindberg Gottlieb,
Denmark
PO-1573
Abstract
Margins based on inter-fractional surgical clip movement for breast tumor bed radiotherapy boost
Authors: Karina Lindberg Gottlieb1, Simon Long Krogh1, Mette Holck Nielsen2, Ebbe Laugaard Lorenzen3
1Laboratory of Radiation Physics, Department of Oncology, Odense University Hospital, Odense, Denmark; 2Department of Oncology, Odense University Hospital, Odense, Denmark; 3Laboratory of Radiation Physics, Department of Oncology; Odense University Hospital, Odense, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
Simultaneous
integrated boost in breast cancer radiotherapy has the advantage, compared to
sequential boost, of shortening the overall duration of the radiotherapy
course. However, during the treatment course the boost target region, typically
identified by surgical clips, may move relative to the other target regions. In
this study, the inter-fraction movement of the surgical clips in the boost region
relative to the remaining target regions was evaluated, and the corresponding
required PTV margins are estimated.
Material and Methods
Daily Cone
Beam CT (CBCT) scans from all patients treated with simultaneous boost between October
2017 and November 2020 were included, yielding 1628 scans from 90 patients. The
registrations done in the clinical workflow were used for this study. The workflow
(illustrated in figure 1) was as follows: First, a boost specific match was performed,
where the surgical clips in the boost region were registered to their position in
the planning CT manually. Then, an automatic match on the chest wall and
lymph-node regions (if present) was performed. We calculated the systematic (Σ) and random (σ) components. Corresponding
required PTV margins were calculated based on a margin formula of 2.5 Σ+0.3 σ.
The constant for σ (0.3)
was based on a boost dose of
63 Gy and a whole breast dose of 51.52 Gy.
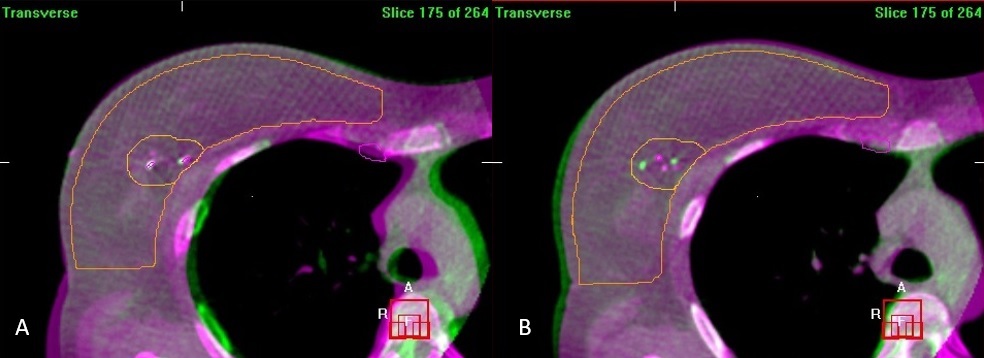
Figure 1. A clinical match of a patient. a)
manual match using the clips and b) automatic match on the chest wall. Purple
is the reference CT and Green is the CBCT.
Results
The
observed displacement of the surgical clips is shown in figure 2 with the corresponding
systematic and random components. The displacement was similar in all
directions with average components of Σ = 1.9mm and σ
= 1.7mm. Based on this the corresponding PTV margin due to inter-fractional
displacement of the clips is 5.2mm. Breathing motion could introduce additional
random errors, but the impact is limited, e.g. an additional random error of
1.5mm would increase the PTV-margin to 5.4mm. Any systematic errors would
increase the margin; however, the value of 1.9mm from clips displacement will
be predominant with typical values, e.g. an additional systematic error of 1mm would
increase the PTV margin to 5.8mm.
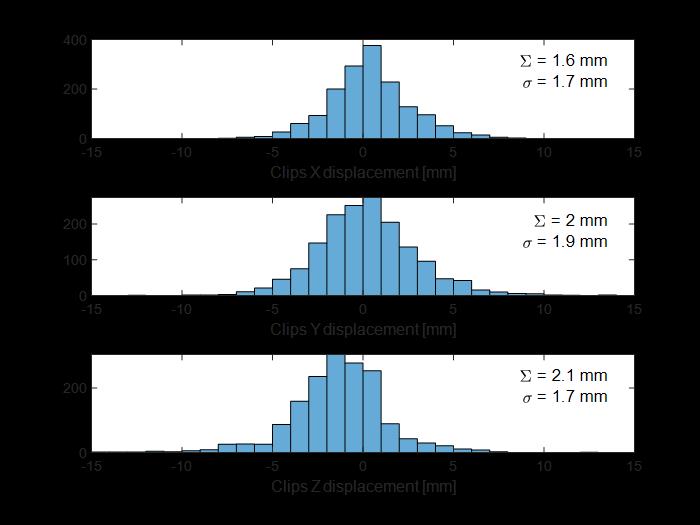
Figure 2. Histogram of the displacement of surgical clips
relative to breast/chest and lymph node target regions as measured on 1682
daily CBCT scans. Corresponding systematic (Σ) and random components (σ )
is shown in each subfigure.
Conclusion
Displacement
of the surgical clips in the boost region is a major uncertainty in simultaneous
integrated boost for breast cancer radiotherapy. However, with the use of daily
CBCT performing a match on breast/chest and lymph node regions, the additional
uncertainty from clips displacement alone can be accounted for by adding a PTV
margin to the boost region of 5mm.