Automated sarcopenia assessment in the neck and survival analysis in head and neck cancer patients
Hermione Warr,
United Kingdom
PD-0783
Abstract
Automated sarcopenia assessment in the neck and survival analysis in head and neck cancer patients
Authors: Hermione Warr1, Olivia Murray1, Dónal McSweeney2, Alan McWilliam2, Andrew Green2
1The University of Manchester, Physics and Astronomy, Manchester, United Kingdom; 2The University of Manchester, Division Of Cancer Sciences, Radiotherapy Related Research, Manchester, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Sarcopenia can be used to quantify the frailty of a patient, and can be assessed by extracting skeletal muscle characteristics. Models have been developed to measure skeletal muscle at the third lumbar vertebra level (L3); however, head and neck cancer scans often do not extend into the abdomen. The purpose of this investigation was to develop a model that automatically extracts muscle characteristics in the cervical spine (C3), and use these to assess head and neck (H&N) cancer patients for sarcopenia, before analysing the impact of depleted skeletal muscle on survival.
Material and Methods
Skeletal muscle at C3 was manually delineated for 35 patients using pre-treatment CT scans from an open database of Head and Neck Squamous Cell Carcinoma (HNSCC) patients. Each patient was segmented by two observers to allow an estimation of interobserver variability.
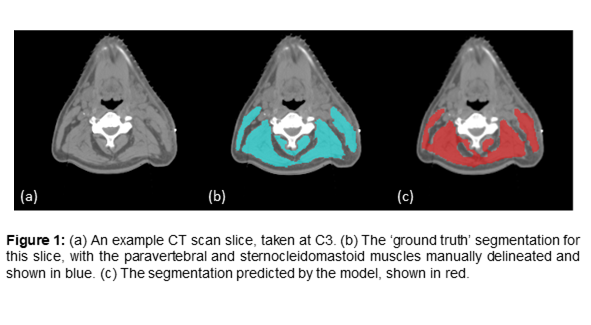
Convolutional neural networks (CNNs) are often used for the automatic segmentation of medical images. Transfer learning is a common technique used when there is limited training data available. A pretrained CNN (FCN-ResNet-50) was fine-tuned to segment the sternocleidomastoid and paravertebral muscles (training=25, testing=5, validation=5), shown in Figure 1.
The model was applied to 189 C3 CT slices. Skeletal muscle area (SMA) and skeletal muscle density (SMD) (mean intensity in HU) were extracted from the segmentations after reviewing model predictions. The impact of these measurements on patient survival was analysed using a multivariate Cox proportional hazards model, with backwards variable selection considering tumour stage, RT total dose, number of fractions, age, sex, surgical intervention and current smoker status.
Results
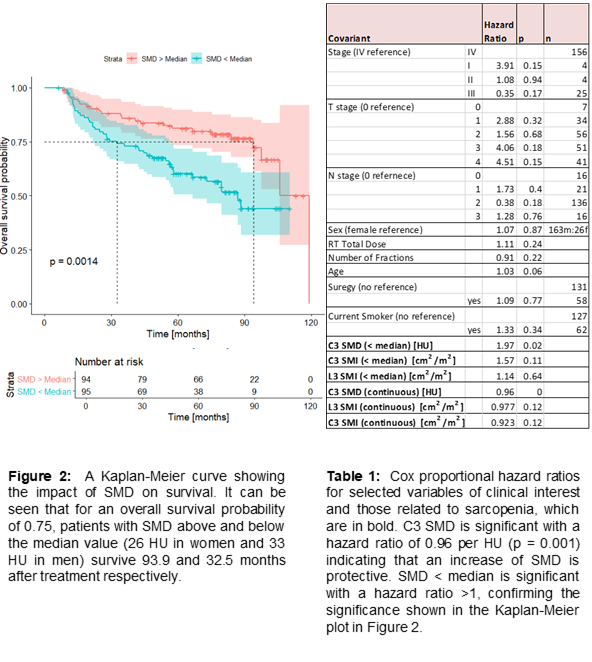
The interobserver Dice score was 0.88, and the network achieved a Dice score of 0.89 indicating it is equivalent to a human observer. Only SMD was found to be prognostic (continuous variable, p = 0.001) in a multivariate model, with a hazard ratio of 0.96 per HU, indicating a decrease in SMD results in a worse patient outcome. The Kaplan-Meier curve for SMD, split by median values for men and women (33 HU and 26 HU), is shown in Figure 2, alongside the Cox regression hazard ratios shown in Table 1. Patients with SMD > median showed a higher survival time than patients with SMD < median, (93.9 months vs 32.5 months) for a survival probability of 0.75, suggesting that skeletal muscle is protective.
Conclusion
An automatic model for determining skeletal muscle characteristics at C3 was developed using a pretrained CNN. The model was used to extract the SMD of 189 H&N cancer patients (median: 26 HU in women, 33 HU in men) and this was shown to be prognostic. The lack of significance in clinical variables indicates the need to explore a larger dataset. Our novel model at C3 allows sarcopenia assessment in H&N cancer patients, who often do not have scans that extend to L3. Further work will develop a suite of models at other vertebral levels to allow sarcopenia assessment of all radiotherapy patients.