Impact of motion compensated reconstruction of 4DCT on radiomic features
Chelsea Sargeant,
United Kingdom
PO-1821
Abstract
Impact of motion compensated reconstruction of 4DCT on radiomic features
Authors: Chelsea Sargeant1, Angela Davey1, Marcel van Herk1, Alan McWilliam1
1The University of Manchester, Division of Cancer Sciences - Faculty of Biology, Medicine and Health, Manchester, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
4DCT is routinely used for imaging early-stage NSCLC patients treated with SABR. With individual 4D phases and reconstructions available, there is uncertainty surrounding the optimal 4DCT image for radiomics. We compare for the first time, the impact of motion compensated (MC) reconstructions with 4D phase selection on radiomic prediction of distant recurrence (DR).
Material and Methods
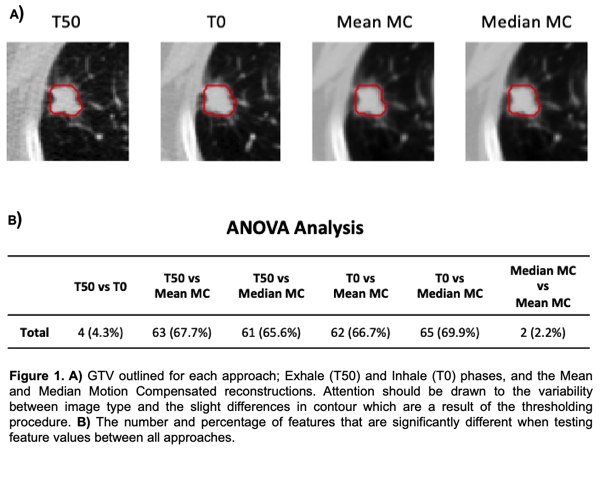
4DCT and follow-up data was collected for 262 NSCLC patients treated with SABR. Patients with tumour volumes ≤2cm³ and missing clinical data were excluded. The 4DCT scan consisted of 10 phases including end of exhale (T50) and peak inhale (T0). In-house software generated Mean and Median MC reconstructions. An in-house validated approach converted the clinical ITV into the GTV on T50, which was rigidly translated to T0 and MC scans before thresholding to provide a better GTV for each reconstruction (Fig.1A).
93 features were extracted from the GTV on each reconstruction using pyRadiomics and directly compared with a one-way ANOVA test. Unsupervised feature selection removed volume-correlated and redundant features, using Spearman’s rank correlation coefficient.
Remaining features were assessed for their ability to predict DR. Bootstrapped univariable Cox analysis was performed and significant features (p<0.05) were included in a multivariable Cox model with variables: tumour volume, tumour motion, lobe location, performance status, age and T stage. Over 500 resamples, selected features were recorded and concordance index (CI) was calculated. Finally, models were built using the top ranked features across resamples, with number of features determined by the median signature size. Each model was assessed in terms of Akaike Information Criterion (AIC) and prognostic features.
Results
223 patients remained in the analysis. Over 60% of selected features differed between image types (Fig.1B). Following feature selection, the percentage of remaining features was: 11%, 13%, 15% and 14% for T50, T0, Mean MC and Median MC.
Median signature length was consistent, and FirstOrder_90Percentile was selected regardless of model. Both MC reconstructions offered virtually the same information.
Overall, T50 (exhale) had the highest number of prognostic features remaining in multivariable analysis (Fig.2A). Fig.2B demonstrates improved performance (higher CI and lower AIC) in the single phase models.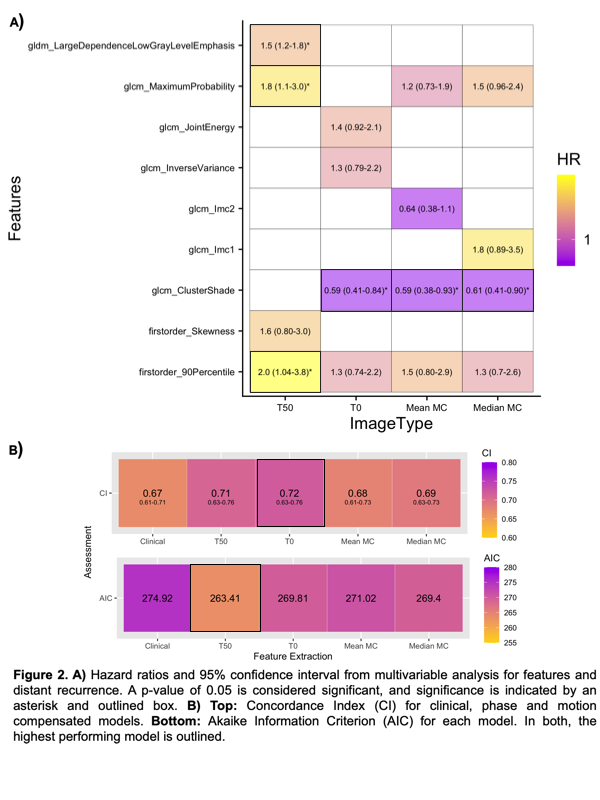
Conclusion
There are significant differences between most images investigated, in feature values and correlations with volume and other features. There is, however, little difference between feature signature for MC scans.
Features were prognostic for DR, and outperformed clinical variables, regardless of image type. However, MC scans offer no improvement over single phase images; the latter produces better prognostic models. Motion compensation reduces noise, but tumour radiomics is more impacted by loss of image detail due to residual motion after deformable registration, e.g. due to registration inaccuracies and cardiac motion.