Surface guided FLASH radiotherapy
Annika Mannerberg,
Sweden
PO-1767
Abstract
Surface guided FLASH radiotherapy
Authors: Annika Mannerberg1, Elise Konradsson1, Malin Kügele1, Anneli Edvardsson2, Crister Ceberg1, Hanna-Maria Thomasson2, Maja L. Arendt3, Kristine Bastholm Jensen4, Sofie Ceberg1
1Lund University, Department of Medical Radiation Physics, Lund, Sweden; 2Skåne University Hospital, Department of Hematology, Oncology and Radiation Physics, Lund, Sweden; 3University of Copenhagen, Department of Veterinary Clinical Sciences, Fredriksberg, Denmark; 4Veterinärhuset Öresund, Limhamn, Malmö, Sweden
Show Affiliations
Hide Affiliations
Purpose or Objective
Ultra-high
dose rate radiotherapy (FLASH-RT) involves few fractions of high doses delivered in a fraction of a second
and aims to widening the therapeutic window by reducing normal tissue toxicity.
Although the fast delivery entails
largely reduced intrafractional motion, it is crucial to have proper motion
management to ensure precise delivery of the high dose. For motion management,
surface guided radiotherapy (SGRT) provides real-time monitoring, sub-millimeter
accuracy and a large field of view (FoV). Rendering of surface images (SI)
requires that the projected light is reflected and detectable by the surface
scanning (SS) system’s camera. In a novel approach, we aim to utilize SGRT
for motion management during FLASH-RT.
Material and Methods
Four canine cancer patients were treated with surface
guided FLASH-RT at a modified linear accelerator (Precise, ELEKTA, Sweden). Prescribed
doses of 28-35 Gy were delivered in 3.5 µs electron pulses (200 Hz) during a
total treatment time of 60-125 ms. The patients were anesthetized prior to
treatment. For SGRT, a single camera (CatalystTM, C-RAD, Sweden)
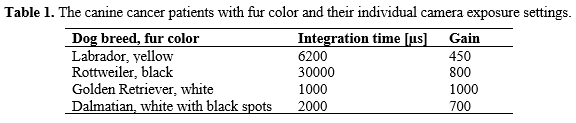
unit was used. To account for the wide range of fur colors, the appropriate integration time and gain was individually set for each
patient to optimize the rendered SI. Also, the FoV was adjusted due to the
off-isocentric treatment. The reference SI was acquired in conjunction with the
patient positioning. Recording of the motion during the whole treatment
session, including the FLASH delivery was executed for one patient. The motion was analyzed by retrieving data
from the SS system log files.
Results
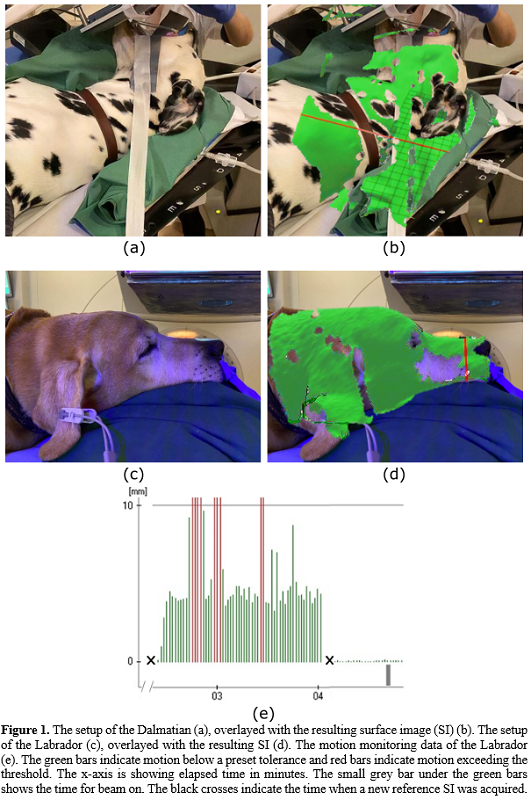
The
individual camera exposure settings for all canine cancer patients and SI for
two of them are presented (Table 1, Figure 1b, 1d). For the patient where surface
guided motion management during beam-delivery was used, motion up to 3 cm between
patient setup and treatment start was recorded (Figure 1e) and treatment was
postponed until full anesthesia was reached. The total vector offset from the
reference SI was 0.1 mm at the time of radiation delivery indicated by the SS
system (Figure 1e). The same offset was also observed 1.72 s before beam-on and
1.63 s afterwards. For patients with very dark
fur, it was challenging to obtain an acceptable SI due to hardware limitations.
When encountering the maximum exposure time, the signal could not be further
amplified which resulted in either a decreased speed of the SS system or decreased
reconstructed surface regions (Dalmatian vs Labrador, Figure 1b and 1d).
Conclusion
We have
demonstrated that motion management during FLASH-RT is important and feasible
using SGRT. It was shown that the surface scanning system can cover the required
FoV and capture images during the off-isocentric FLASH-RT treatment. It can be
used to estimate the motion prior to treatment and to assure that the patient remains
in the correct position during beam delivery.