Patient positioning and intrafraction movement control protocol using an IGRT and SGRT system in SRS
María Pinto Monedero,
Spain
PO-1743
Abstract
Patient positioning and intrafraction movement control protocol using an IGRT and SGRT system in SRS
Authors: María Pinto Monedero1, Ruth Rodríguez Romero1, Patricia Sánchez Rubio1, Jaime Martínez Ortega1, Arturo López Corella 1, Miguel Torres López1, Julia Ciudad Roca1, Ana María Lloret Gudiña1
1Hospital Universitario Puerta de Hierro Majadahonda, Medical Physics Department, Madrid, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
Surface guided radiotherapy (SGRT) monitors patient position through its surface during treatment, complementing image guidance. Stereotactic radiotherapy treatments (SRS) requires submilimetric accuracy and precision.
The purpose of this work is to describe a protocol for patient positioning and intra-fraction movement control in SRS treatments using a SGRT system complementing radiographic image, which has allowed to achieve an accuracy and precision in treatments comparable to the system previous existing in the center (<0.3mm, 0.3 °)
Material and Methods
SRS technique was previously performed using a Novalis linac (Brainlab, Germany) and IGRT ExacTrac system with 6D robotic couch (Brainlab), which allowed image control using orthogonal X-ray images, for any combination of couch and gantry rotation. Closed masks were used for radiosurgery (Brainlab) and accuracy <0.3 mm, 0.3 ° was achieved.
SRS technique has been implemented using a TrueBeam HD120MLC with a 6D robotic couch (Varian Medical Systems, USA) and an AlignRT surface guidance system (VisionRT, UK). AlignRT monitors the patient's surface throughout the treatment by comparing it, with six degrees of freedom, with the reference surface from the CT simulation. Also, a CBCT can be performed with the table at 0 °, but not when couch is rotated. The masks used for immobilization of the patient are open Encompass SRS Fibreplast (Q-Fix, USA).
Results
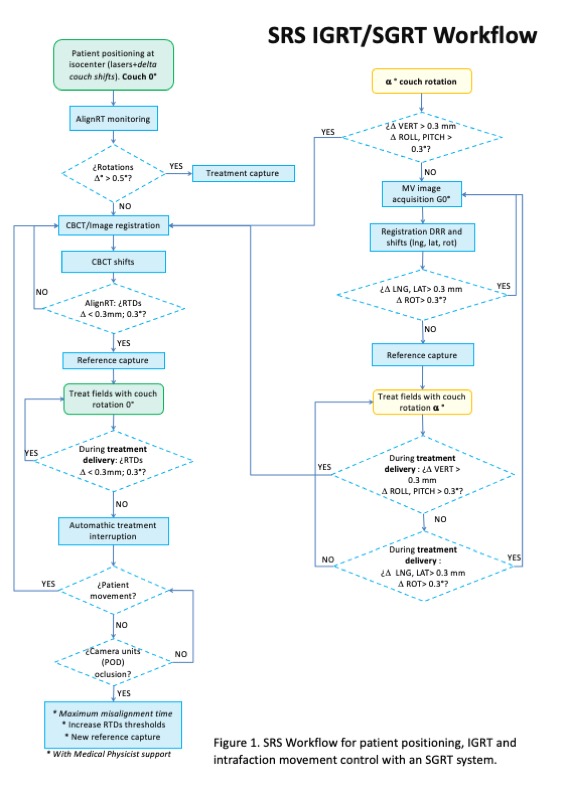
SRS workflow is summarized in Figure 1. After positioning the patient at the isocenter, AlignRT monitors the patient surface. Initial deviations from the reference surface> 0.5mm, 0.5 ° are corrected by acquiring a treatment capture. A CBCT is performed with couch rotation 0 °, then image registration, and the corrections are applied with 6 degrees of freedom. If AlignRT showed discrepancies greater than tolerance (0.3mm, 0.3 °), the CBCT would be repeated; otherwise, a reference capture is acquired, and fields with couch rotation 0 ° are treated. For each beam with different couch rotation, an AP portal image is taken to correct deviations in longitudinal, lateral and rotation until they are within tolerance. If the deviations were vertical, roll or pitch, the CBCT would be repeated with couch rotation 0 °. If all deviations are within tolerance, a new reference capture is acquired and beams treated.
If during treatment any threshold is exceeded and there is suspicion of patient movement, the CBCT would be repeated with couch rotation at 0 °. If the occlusion of one of the cameras (POD) is responsible for the discrepancies, support of the medical physicist is required to assess a temporary opening of the tolerance or an increase in the maximum allowed deviation time.
Conclusion
The presented treatment and intrafraction movement control protocol have allowed the implementation of the SRS technique while maintaining the precision and accuracy of 0.3mm, 0.3 °.