Commissionning of iterative model reconstruction (IMR) on Philips BigBore CT Scanner
Gregory Bolard,
Switzerland
PO-1669
Abstract
Commissionning of iterative model reconstruction (IMR) on Philips BigBore CT Scanner
1Hôpital de La Tour, Radiation oncology, Meyrin, Switzerland
Show Affiliations
Hide Affiliations
Purpose or Objective
Purpose of this work is to evaluate the benefit in the scope of
radiation therapy planning of IMR, a model-based iterative reconstruction
algorithm newly released by Philips for Big Bore CT version 4.8 with the
promise of significative noise reduction. Image quality improvements were
assessed for both standard and 4D reconstructions.
Material and Methods
Spatial resolution, noise and low contrast detectability were measured
at 120 KV using a Catphan 604 phantom for the three
levels of noise reduction (1, 2, 3) and the two image definitions (Soft Tissue,
Routine) offered by IMR (FOV 26cm, slice width 2mm, pitch
0.813). These metrics were compared to the current first generation iterative algorithm used clinically (iDose). Standard deviation a in 20mm
diameter circular ROI was used as noise indicator while MTF at 50% and 10% were
calculated for spatial resolution assessment. The largest low contrast rod (nominal
1.0%) was used for contrast calculation. HU to relative electron density stability was evaluated using a CIRS model 062 phantom. For 4D
acquisitions (helical acquisition at low pitch), the same Catphan phantom was
moving using a dynamic platform during X-ray following a periodic
cos4 pattern (20mm amplitude, period 4s) in the superior-inferior direction.
Results
IMR exhibits higher spatial resolution and better low contrast
detectability than iDose for the same exposure. Spatial resolution is nearly independent
of noise level reduction and exposure and is respectively 1.35 and 1.1-times
higher than iDose (level 4, filter B) for image definition routine and soft
tissue. IMR1 show similar noise level than iDose (level 4) while IMR2 and 3
provide respectively 33% and 59% noise reduction in average leading to 1.5 and
2.4-times higher contrast. The benefit of this contrast restitution relative to
iDose increases while slice thickness decreases (1.36 at 3mm slice thickness
and 1.63 at 1mm).A similar low contrast detectability and an improved spatial resolution
is achievable with a dose reduction factor of 4 with IMR2 routine and 5 with
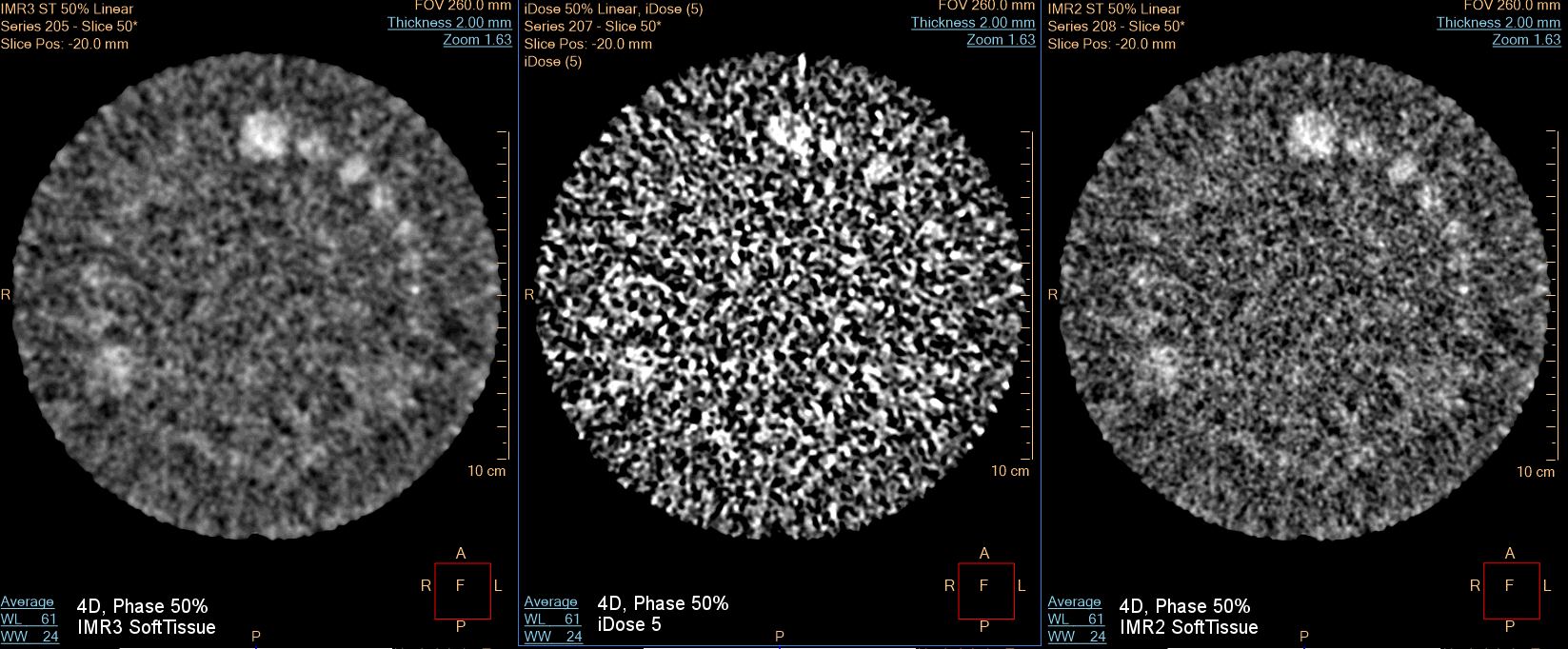
IMR3 routine.Significative low contrast detectability improvements are observed for 4D
reconstruction (phase binning, bin width 10%) with Soft IMR level 2 or 3 image
definition soft tissue, with 1% contrast now visible above CTDI of 14mGy. HU are not influenced by IMR level or image definition type and HU to mass density relationship is nearly identical to iDose which facilitates the clinical
adoption for dose calculation.
Conclusion
For a given dose
level, the knowledge-based reconstruction algorithm IMR can improve both spatial
resolution and low contrast detectability in comparison to iDose, improving
overall image quality. IMR advantages relative to iDose increase when
decreasing slice thickness and exposure. IMR 2 or 3 Tissue image definition
significantly improve low contrast detectability for 4DCT acquisitions, parameter
of interest in the abdomen area. HU numbers do not depend on image definition
and noise reduction level and are similar to iDose.