Inverse Consistency Error for quantifying uncertainty in DIR: validation on three different sites
PO-1658
Abstract
Inverse Consistency Error for quantifying uncertainty in DIR: validation on three different sites
Authors: Marco Fusella1, Christian Fiandra2, Marica Vagni3, Nicola Michielli3, Alessandro Scaggion4, Claudio Vecchi5, Stefania Zara5, Filippo Molinari3, Gianfranco Loi6
1Veneto Institute of Oncology - IOV IRCCS, Medical Physics, Padova, Italy; 2University of Turin, Department of Oncology, Radiation Oncology, Turin, Italy; 3Politecnico di Torino, PoliToBIOMed Lab, Biolab, Department of Electronics and Telecommunications, Turin, Italy; 4Veneto Institute of Oncology IOV-IRCCS, Medical Physics Department, Padua, Italy; 5Tecnologie Avanzate T.A. Srl, R&D, Turin, Italy; 6University Hospital Maggiore della Carità, Department of Medical Physics, Novara, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
To assess the performances of a novel automatic approach
based on a voxel-based measure, the Inverse
Consistency Error (ICE), to evaluate the accuracy of the Deformable Image Registration (DIR)
in clinical practice.
Material and Methods
The ICE was computed directly from the deformation
vector field (DVF) provided by the Treatment Planning System (TPS). In order to verify the results obtained from the ICE analysis, the
ground truth was generated through three digital phantoms based on real Head-Neck, lung and
pelvis patient datasets; DVFs were produced by ImSimQA mimicking clinical observed
anatomical changes during treatment. For each site, from the original datasets,
two different DVFs were generated, simulating different level of organs changes
and motion [1]. All Regions of Interest (ROIs) contoured by Medical Doctors (MDs) in the
reference datasets were generated using the same DVFs as reference; they were
then imported and registered in RayStation TPS. All generated DVFs were
exported making them comparable by rescaling the deformation grids and the
intensity values. The ICE, Mean Distance to Conformity (MDC) and Conformity
Index (CI) were computed for each mapped ROI. From ICE distribution were
extracted mean, max, median and the four percentiles. Then CI and MDC standard
metrics (described and analyzed in previous studies [1,2]) were correlated with
the ICE parameters.
[1] https://doi.org/10.1002/mp.12737
[2] https://doi.org/10.1016/j.prro.2019.11.011
Results
Analyzing the data obtained from a total of 68 ROI,
any statistically significant difference was found in terms of applied DVF for
all metrics. Significant differences (p<0.05) were found between sites (lung
differs from the others) for all analyzed metrics. Carrying out a multilinear
regression between MDC, IC and ICE parameters the mean value of ICE (ICE_mean)
resulted a significant predictor of MDC (p=0.0121). Figure 1 represents the
correlation between ICE_mean and MDC. As shown by the Bland-Altman plot in
Figure 2 ICE-mean predicted MDC with a precision inferior to the voxel size (3
mm). Even if a bias of 1.27 mm was found between the metrics setting a threshold of 3 mm (sub-voxel
accuracy) the True Positive Ratio resulted 0.97.
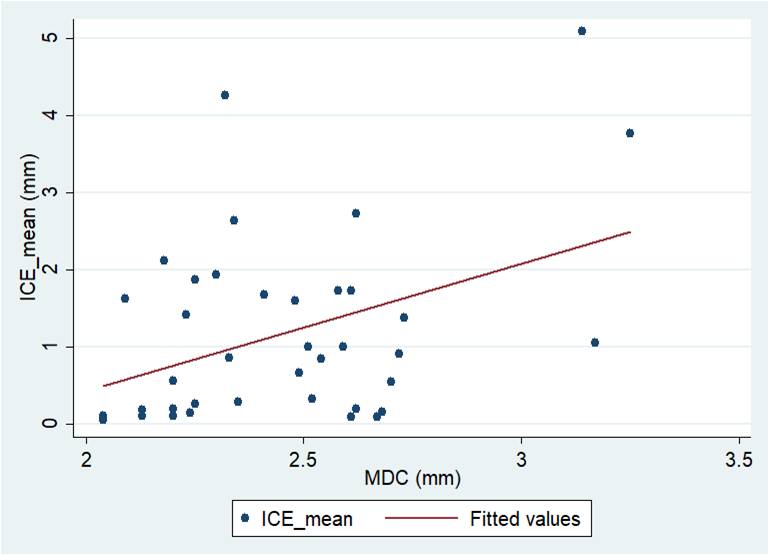
Figure 1. Correlation
between ICE_mean and MDC.
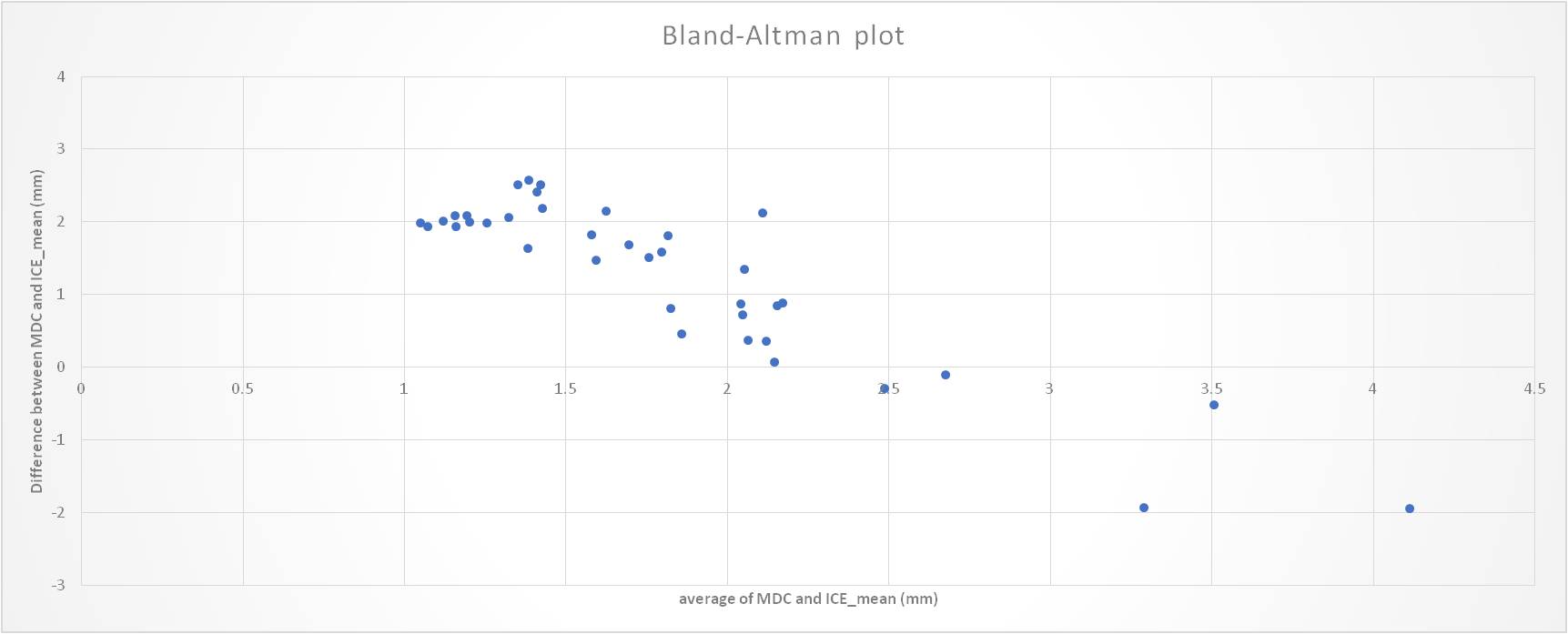
Fig.2 Bland-Altman
plot showing the limits of agreements (LOA) between ICE_mean and MDC. The LOA were inferior than 2.2 mm
(ICE-mean predicts MDC with sub-voxel precision).
Conclusion
This study represents the first comparison between
contour based and volumetric metrics for DIR validation.
The results indicate that in the presence of
clinically consistent deformation, ICE is a valuable indicator for
patient-specific DIR verification. Associated with known and used metrics (such
as MDC) at sub-voxel accuracy, ICE adds a volumetric information that generally
lacks in previous studies representing a promising tool for quantifying
uncertainty in the DIR process. Further developments will focus on validating
these findings in a multicenter scenario.