For the
CBCT, the distance observed between the four radiopaque markers differed less
than 0,1 mm from their real value. Neither did the grid analysis show
appreciable distortion. The mean value (µ) and standard deviation (σ) of the grid size were 0,34 +
0,24 mm and 0,36 + 0,36 mm for horizontal and vertical direction,
respectively. It should be noted that the image in the upper area of the grid
was diffuse, probably due to the off-axis location of the phantom and the
conical geometry of the beam.
The volumes
obtained by automatic segmentation differed between 1,6 and 5,6% from the
nominal values provided by the manufacturer.
The results
of the comparison between the CBCT angiography and the CT simulator, based on
the analysis of the CATPHAN phantom images are shown in Fig. 2.
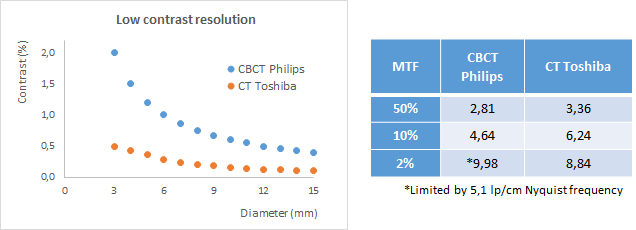
Fig. 2. CBCT
vs CT-simulator results comparison with CATPHAN phantom.
The
limitation given by the CBCT pixel size (0,98 mm) prevented meeting the usual
tolerance for head CT examinations of 6 lp/cm at MTF 2%.
Although the low-contrast resolution of the CBCT was
worse, both 3D imaging modalities met the usual tolerances: 3% and 0,8% for 3,5
and 8 mm diameter objects, respectively.