Dose-escalated pencil beam proton therapy for reirradiation of pelvic recurrences from rectal cancer
Camilla Kronborg,
Denmark
PO-1271
Abstract
Dose-escalated pencil beam proton therapy for reirradiation of pelvic recurrences from rectal cancer
Authors: Camilla Kronborg1, Heidi Staghøj Rønde1, Jesper Folsted Kallehauge1, Marianne Grønlie Guren2, Kare-Lise Garm Spindler3
1Danish Centre for Particle Therapy, Danish Centre for Particle Therapy, Aarhus N, Denmark; 2Oslo University Hospital, Department of Oncology, Oslo, Norway; 3Aarhus University Hospital, Department of Oncology, Aarhus N, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
Up to 10% of patients with rectal cancer have a pelvic
recurrence after surgery. As pre-operative radiotherapy is an integrated part
of the primary treatment for advanced cases many have received radiotherapy as
a part of the initial strategy.
Surgery is the main treatment for pelvic recurrence,
and outcome is highly dependent on radical (R0) resection. To increase R0 resection rate,
re-irradiation has been introduced, mainly with doses around 40 Gy, with
manageable toxicity. Tumor control probability studies indicate,
that doses around or above 50 Gy are associated to better pathological
response. Additionally, not all recurrences are eligible for surgery, in these
instances low dose radiotherapy or palliative systemic treatment is often
applied.
A comparative planning
study was performed to determine if dose escalation with pencil beam proton therapy
was feasible for pelvic recurrences of rectal cancer
Material and Methods
Previously irradiated patients, with
pelvic recurrences from rectal cancer, treated according to a re-irradiation
protocol (40.8 Gy, 1.2 Gy per fraction, twice daily and concomitant capecitabine) were selected for comparative proton planning. The clinical
photon plans were done with 1 or 2 arcs (VMAT), Eclipse. Proton plans were done
with 3 posterior field robust IMPT planning (Multi field optimization, Eclipse
v13.7) to 40.8 Gy RBE, 55 Gy RBE or 65 Gy RBE.
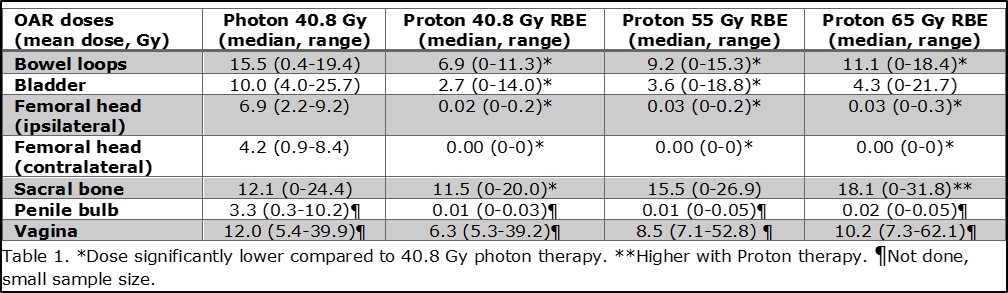
OARs were delineated according to RTOG
guidelines. Dose to OARs (bowel loops, bladder, femoral heads, sacral bone,
penile bulb, vagina) where compared for photon vs. doseescalated proton plans.
For comparison of selected DVHs metrics
Wilcoxon's signed ranks test was used. A p-value<0.05 was considered
statistically significant.
Results
Eight patients were included (50% male), time to
re-irradiation was 4.1 years (range: 2.2-6.9). Re-irradiation volumes (CTVs)
ranged from 84 cm3 to 1080 cm3.
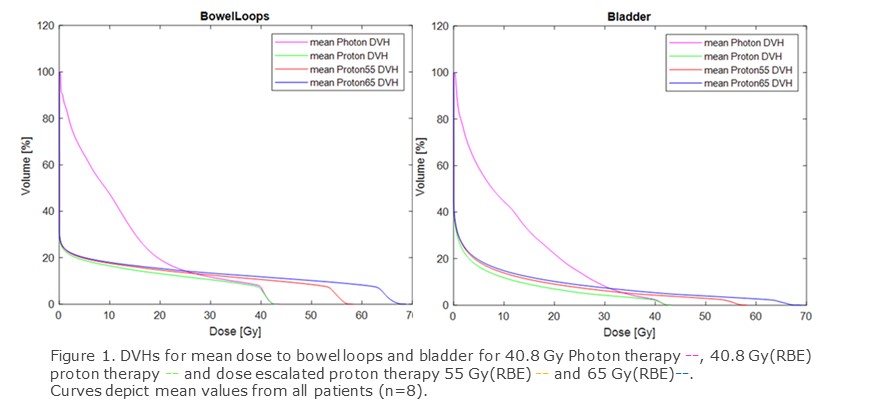
Mean dose to all OARs was lower with 40.8 Gy proton
vs. 40.8 Gy photon therapy. Comparing dose escalations to the 40.8 Gy photon
plan, mean dose to bowel loops was still significantly lower with dose
escalation to 55 and 65 Gy, both p<0.01. Mean bladder dose was
lower for both dose escalations, but only significantly for 55 Gy p=0.04 and
p=0.055. For ipsi- and contra lateral femoral head, mean doses were
significantly lower despite dose escalations, all p<0.01. Mean
sacral dose was similar for the 55 Gy escalation plan but higher for the 65 Gy
plan p=0.17 and p=0.05, fig 1 and 2. Due to small
numbers statistical comparison was not done for penile bulb and vagina, but
organs were generally spared with proton plans. As expected max doses increased
for OAR close to or in the CTVs.
Conclusion
Dose escalation to 55 or 65 Gy RBE for
re-irradiation of pelvic recurrences is possible while keeping mean doses to
OARs at lower or similar levels as 40.8 Gy photon plans. Dose escalation could
be relevant for both increasing radical resection in resectable recurrences or
as a definitive treatment for unresectable recurrences.