Inhomogeneous dose escalation in pancreatic SBRT:feasibility and impact of anatomical configuration
PO-1226
Abstract
Inhomogeneous dose escalation in pancreatic SBRT:feasibility and impact of anatomical configuration
Authors: Mauro Loi1, Raffaela Doro2, Sara Lucidi1, Pierluigi Bonomo1, Gabriele Simontacchi1, Daniela Greto1, Andrea Allegra1, Vanessa Di Cataldo1, Giulio Francolini1, Ivano Bonucci2, Lorenzo Livi3, Laura Masi2
1Azienda Ospedaliero-Universitaria Careggi, Radiation Oncology Unit, Florence, Italy; 2IFCA, Department of Medical Physics, Radiation Oncology, Florence, Italy; 3Azienda Ospedaliera Universitaria Careggi, Radiation Oncology Unit, Florence, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
In
non-resectable locally advanced pancreatic cancer, adjunction of Stereotactic
Body Radiotherapy (SBRT) following chemotherapy has been proposed to improve
outcome. However, prescription of more intensive schedules has been
traditionally limited by risk of severe injury to nearby organs at risk (OARs),
particularly in case of substantial overlap between planning volume and
critical structures. To achieve higher tumor control probability, a
biologically effective dose (BED) of 100
Gy10 , corresponding to a dose 50 Gy in 5 fractions of 10 Gy
assuming α/β=10, is desirable. The aim of our in-silico study is to assess
the feasibility of dose escalation using inhomogeneous dose prescription for
pancreatic SBRT and to determine which patients may be eligible for this
strategy based on anatomical proximity between target volumes and OARS.
Material and Methods
Data from 14
locally advanced pancreatic cancer patients treated at our Institution were
collected. For each patient, a CyberKnife (CK) Synchrony treatment plan was optimized
for fiducial-guided pancreatic SBRT aiming at a planned dose of 50 Gy and 40 Gy
in 5 fractions to the gross tumor volume (GTV) and the planning target volume
(PTV), respectively. PTV was created by 5 mm GTV isotropic expansion. Acceptable
target coverages were: 1) a dose of 50 Gy and 47.5 Gy to at least 90% and 95%
of the GTV, and 2) a dose of 40 Gy to
95% of the PTV. Planned doses to the target regions and OARs (duodenum, stomach
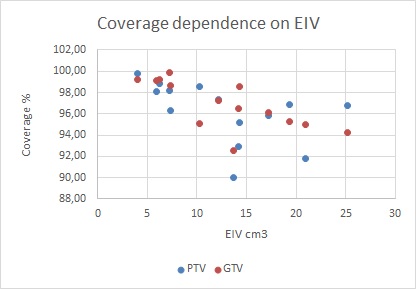
and bowels) were evaluated and statistically analyzed. For each plan, the intersection
volume between the PTV and OARs expanded by 5 mm was defined as Expansion-Intersection
Volume (EIV), as reported by Tomatis et al.
Results
Median GTV and
PTV volumes were 40.8 (range 22.3-205.3) cc and 73.7 (range 36.1-266.7) cc ,
respectively. V35 to duodenum, stomach and bowel was maintained below 0.5 cc in
all cases. Median EIV was 12.9 (3.9-25.1) cc. Median V50 and V47.5 for GTV was
91.0% (range 82.4%-97.8%) and 96.8% (range 92.5%-99.9%), respectively: GTV coverage
was acceptable in 10 out of 14 cases. Median V40Gy for PTV was 96.8%
(range 90.0%-99.8%): PTV coverage was acceptable in 11 out of 14 cases.
Spearman correlation showed a significant association between EIV and V47.5Gyfor
GTV (rho -0,77228, p<0.001) and V40Gyfor PTV (rho -0,68352, p<0.001), respectively.
Conclusion
Inhomogenous
dose escalated prescription using fiducial-based SBRT with Cyberknife respiratory
tracking is a feasible strategy in selected patients with locally advanced
pancreatic cancer. EIV, but GTV size, is significantly correlated with
target coverage probability and may provide a simple tool to identify patients
eligible for dose escalation.